







feature
Continuum of Care: The Capsular Tension Ring
CTRs
can be an important part of your arsenal, but they must be used judiciously.
BY ROBERT OSHER, M.D.
Capsular tension rings (CTRs) are effective adjunctive devices that can convert a potential catastrophic phaco procedure into a success story. Surgeons can avert complications associated with weakened zonules, and in turn, elevate the standard of care for their cataract patients.
And while this technology has been available to American surgeons since the early 1990s, I am often surprised by the number of surgeons who do not feel comfortable using a CTR. I am also somewhat perplexed to hear about surgeons who implant CTRs for virtually every reason. With possibly some confusion about the issue, I will discuss when some patients' physical characteristics and also certain intraoperative situations may warrant ring utilization.
|
|
|
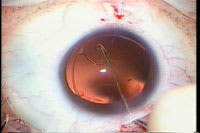
The Cionni Capsular Tension Rings may be fixated to the sclera. |
Making the Case for CTR
I recall at a meeting years ago, a surgical colleague accosted me when I candidly stated that the approval of the capsule tension ring by the FDA instantly changed the standard of care. Referring back to the analogy, would the same surgeon believe that a Weck cell vitrectomy was within the standard of care?
We take an oath that we will not harm the patient and it is our responsibility to deliver the care that has been clearly shown to yield the best and safest results. Managing vitreous without a vitrector or managing a zonular dialysis without the availability of a CTR may prove detrimental to the patient.
The availability of the CTR is essential during phaco procedures. One never knows when an unforeseen complication will occur, and the best management consists of knowledgeable preparedness.
Of course, any complication, even if perfectly managed, may result in a suboptimal outcome. Moreover, every case of weak zonules does not require a CTR. Yet the surgeon should be familiar with the device and it should certainly be available whenever he or she performs cataract surgery.
Overutilization is always difficult to evaluate, but I do not believe that every high myope or every patient with evidence of pseudoexfoliation should have a CTR implanted when there is no evidence of either zonular weakness or dialysis. I recognize that we are seeing more cases of late IOL-capsular bag subluxation years after uneventful surgery, but there is no evidence to suggest that implanting a CTR within the capsular bag will prevent progressive zonular damage. While it has become very easy to inject a CTR into a capsular bag distended with an ophthalmic viscoelastic device, there is still a slim chance of a CTR-related complication.
Careful Examination
So when is the use of a CTR clearly indicated? During the initial examination, some different pre-existing physiological indicators might suggest patients have zonular weakness, and a CTR, such as StabilEyes (AMO), might be more likely necessary.
There are a number of subtle biomicroscopic findings that we have published, which may tip off the examiner that the zonules are going to be a problem in surgery. These include the iridolenticular gap sign, which is based upon the detection of a space between the anterior lens capsule and the border of the iris at the pupil. A gap may signify focal zonular loss that has caused a slight posterior tilting of the lens or microsubluxation.
A decentered nucleus can also indicate zonular weakness. This sign can be detected if the examiner can observe the cross-sectional anatomy of the lens with the slit beam when the patient's eye is in the primary position. Focal zonular loss may alter the usual symmetry of forces applied to the lens and result in a subtle shift of the lens away from the area of zonular compromise.
A focal rupture of the zonules can sometimes be identified by lines of vitreous traction. The vitreous can herniate forward through the zonular opening into the posterior chamber. However, it may not be visible through the pupil. A focal zonular rupture should be suspected when the vitreous appears "tented" toward the anterior segment.
Focal iridodonesis can be observed as a subtle shimmering of the iris that is limited to several clock hours corresponding to adjacent zonular disruption. The loss of the barrier effect of the zonules allows the vitreous gel to move forward and contact the iris. As eye movements cause the gel to quiver, the overlying iris shimmers.
Another sign of zonular weakness is the visibility of the lens equator when the patient's gaze is eccentric. Indirect ophthalmoscopy may confirm a microluxation of the lens that can be easily overlooked if the examiner only observes the anatomy of the lens in the primary position.
Further Zonular Weakness Clues
In any patient with pre-existing trauma, there is the possibility that the surgeon will encounter either zonular weakness or a dialysis during surgery. There is probably even a greater likelihood of needing a CTR when operating upon any mature brunescent cataract because there is less tolerance for any movement of the lens.
Certainly, a CTR might be necessary when the patient shows evidence of pseudoexfoliation syndrome. There is an increased risk of a sector zonular defect in cases with congenital coloboma of the iris. I also believe there is an increase in weakness of the zonules in patients with retinopathy of prematurity or retinitis pigmentosa. Of course, patients with Marfan syndrome and other rare conditions like Weil-Marchesani syndrome always have weak zonules.
If obvious phacodenesis is present, or if the lens is markedly subluxed, it is unlikely that a standard CTR will suffice. In these cases, the Cionni Capsular Tension Ring or an Ahmed Segment Ring (both Morcher/FCI Ophthalmics, Marshfield Hills, Mass.) may be necessary. The Cionni CTR possesses a small eyelet that surgeons can utilize in these challenging cases.
Preparedness
Unfortunately, even a meticulous examination will fail to reveal every case of pre-existing zonular weakness. Recently, I encountered a patient who had undergone previous intraocular surgery and I was surprised to find a very loose capsular bag. Even if we could diagnosis every case of pre-existing weak zonules, there is always the possibility of an iatrogenic dialysis. In other words, being prepared is to expect the unexpected. The cataract surgeon should always have quick access to a CTR whenever he or she operates.
Robert H. Osher, M.D., is a professor in the Department of Ophthalmology, University of Cincinnati College of Medicine and medical director emeritus, Cincinnati Eye Institute. Dr. Osher is a paid consultant for AMO. He can be e-mailed at rhosher@cincinnatieye.com.