







Office and Minor Procedures for Ocular Surface Disease
These strategies can prevent the need for more aggressive surgery.
BY CHRISTOPHER J. RAPUANO, MD
OCULAR SURFACE DISEASES are very common in clinical practice, and we have at our disposal a variety of first-line medical treatments we can employ. For patients who don’t respond to medical treatment, office and minor surgical procedures can be extremely effective and often allow us to delay or avoid more aggressive surgeries. Here, I briefly describe a few such scenarios.

We can treat with shave excisional biopsy, cautery, cryotherapy or curettage. Curettage can usually be performed without anesthesia. Using a small chalazion scoop, #15 blade or jeweler’s forceps, core out the central umbilication, enough to cause bleeding. This works very nicely. The lesion usually disappears in a couple of weeks, and the follicles go away in approximately 4 to 6 weeks.
I often choose conjunctival cautery, which can be performed in an exam room chair or minor surgery setting. I balloon up the superior conjunctiva with local anesthetic (e.g., lidocaine). This is helpful because it moves your cautery application away from the sclera. I then use a handheld, battery-operated unit to apply cautery to the superior conjunctiva (Figure 1). Obviously, we need to have a cooperative patient to safely perform this procedure. Patients tend to be a little uncomfortable but not too terribly, and the conjunctival defects typically heal within a week. The results may not last indefinitely, but patients’ symptoms improve significantly.
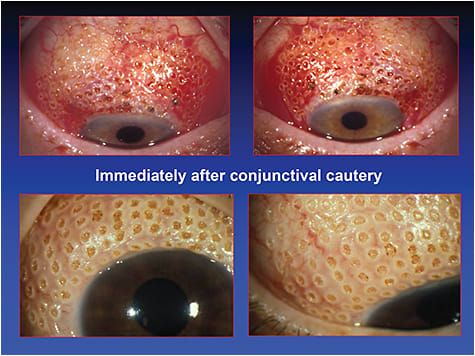
FIGURE 1. Conjunctival cautery is an effective in-office treatment for superior limbic keratoconjunctivitis.
Slightly different, easier-to-use, platforms for in-office use are also available. AmbioDisk (IOP Ophthalmics, www.iopinc.com/store/ambiodisk), for example, can be retained on the ocular surface with a bandage contact lens rather than glue or sutures. Prokera (BioTissue, www.prokerainfo.com) is another in-office option that works well. Prokera is a piece of amniotic membrane tissue held in between two clear, flexible plastic rings, which holds itself in place on the ocular surface. The rings are slightly thicker than an average contact lens, so patients may be aware of the device’s presence, but most are fairly comfortable.
I recently had a patient come to my practice with corneal melt after having a third DSEK done elsewhere. In one area of the cornea, the stroma melted nearly all the way down to the DSEK plane. It just was not healing until we inserted a Prokera. Once we did, the defect healed nicely over the next several weeks.

Christopher Rapuano, MD, is director of the cornea service and co-director of the refractive surgery department at Wills Eye Hospital and a professor at Jefferson Medical College Philadelphia. |