







The Driving Forces in Amniotic Membrane Transplantation
HC-HA/PTX3 helps amniotic tissue reduce inflammation and promote regeneration.
BY SCHEFFER C.G. TSENG, MD, PHD
WHEN CORNEAL TISSUE IS DEGENERATED, AGED, INJURED OR SCARRED, the conventional wisdom is to say, “There’s nothing we can do except give you a surgical allograft.”
Over a decade ago, we learned that the amniotic membrane has the power to promote regeneration in these cases. Amniotic membrane transplantation can deliver anti-inflammatory, anti-angiogenesis, anti-scarring and sometimes anti-adhesion properties. It also offers pain relief for bullous keratopathy and pterygium surgery, and we use it as a substrate or adjuvant in stem cell expansion.
Twelve years ago, my colleagues and I asked the question, What is in amniotic tissue that creates these amazing results? Between 2002 to 2013, we generated several papers about anti-scarring and anti-inflammatory properties, as well as six papers about a factor called HC-HA/PTX3.

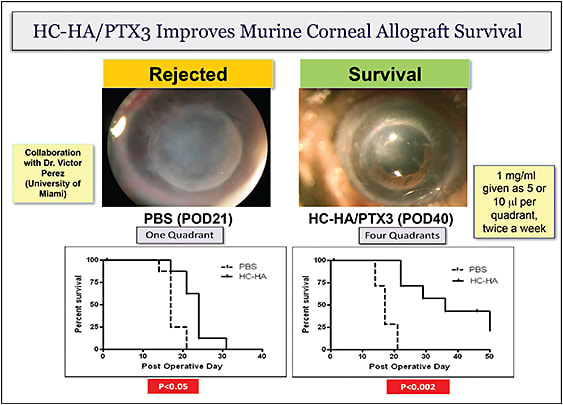
FIGURE 1. HC-HA/PTX3 is able suppress inflammatory responses in vivo by modulating both innate and adaptive immunity of macrophages and CD4(+) T cells. (from He H, Tan Y, Perez VL, Tseng SCG. In vivo downregulation of innate and adaptive immune responses in corneal allograft rejection by HC-HA/PTX3 complex purified from amniotic membrane. Invest Ophthalmol Vis Sci, 55:1647-56, 2014.)
Today, we can say in short that HC-HA/PTX3 is a unique matrix. It only exists two times in life: at ovulation and pregnancy. All of its aforementioned effects are necessary for conception and pregnancy to succeed. Two exciting actions, in my opinion, are anti-inflammatory and regenerative.
This raises two questions: 1) Is our inability to have regeneration related to this three-phase pathway? 2) Within this cascade of cellular infiltration, how do cells interact with each other to generate the final outcome?
When we take a closer look at the macrophage that bridges the neutrophil and lymphocytes (innate and adapted immunity), we find that it selects whether to trigger acute or lingering inflammation or abort. Macrophages have two major phenotypes: the pro-inflammatory M1 and the anti-inflammatory M2. During a wound’s inflammatory stage, polymorphonuclear neurtrophils (PMNs) arrive and promote M1 macrophages. When inflammation is under control, M1 macrophages transform to M2, which promotes wound healing. In the disease state, however, PMNs linger for too long, and the M1 macrophage will activate T cells to lead to chronic inflammatory or non-healing states. For an allograft, that leads to rejection.
It turns out that the successful transition from M1 to M2 macrophage is the key for wound healing. Without it, we have a non-healing wound, such as a diabetic foot ulcer. We have reported that HC-HA/PTX3 can push the PMNs into apoptosis and polarize M2 macrophages.
What’s more, when we converted the cells to myofibroblasts and exposed them to HC-HA/PTX3, they turned to neural crest cells. Finally, we were able to convert those neural crest cells to corneal endothelium. This means that we now know a way to engineer tissue by reprogramming a differentiated or degenerated cell to a progenitor cell. This strategy allows us to engineer autologous tissue, and may one day result in new treatments.
HC-HA/PTX3 is indeed the unique regenerative matrix component from the amniotic membrane. This single molecular complex explains the very potent mystery of how at its center, one agent performs multiple actions.

Scheffer C.G. Tseng, MD, PhD, is Chief Scientific Officer at TissueTech, Inc., and Medical Director of the Ocular Surface Center, Ocular Surface Research and Education Foundation in Miami. |