







I take care of a number of patients with complex anterior segment abnormalities, such as problems relating to the intraocular lens, iris, lens capsule, or zonular fibers. While it is essential to have the right tools for the simplest cases, it is even more important for the complicated ones; consequently, I take advantage of microsurgical instruments, iris hooks, Malyugin rings and capsule support retractors. Without question, small tools can offer big help, as the following cases highlight.
CASE #1: ANTERIOR CAPSULE LACERATION
Just one hour before I saw this patient, she was being treated for a recurrent submacular choroidal neovascular membrane. She had received repeated antivascular endothelial growth (VEGF) factor injections, but had retained good central visual acuity. However, on the particular morning I saw her, her IOP was elevated after the retinal surgeon had injected the medication into the vitreous. The surgeon inserted a 30-gauge needle at the limbus to lower the IOP; an inadvertent laceration of the anterior capsule appeared (Figure 1a). The posterior capsule remained intact.
It could be argued in such cases that it is perhaps better to take a “wait and watch” approach. However, my concern was that any change in the lens material might severely challenge our ability to manage the anterior capsule at surgery. Given the peripheral location of the capsule defect I could not use the femtosecond laser; however, I could rely on micro-instruments.
After capsular staining and under a ophthalmic viscoelastic device (OVD), I went through a nasal paracentesis. Using Seibel capsulorhexis forceps (MicroSurgical Technology, Redmond, WA), I was able to move the capsulotomy back in the direction from which it came, employing Brian Little’s maneuver. As a result, I could start the capsulorhexis without it going further into the zonule. Then, coming around from the far side and back into the nasal paracentesis, I completed a continuous (but not circular) anterior capsulotomy. Six months later the patient was doing perfectly well (Figure 1b).

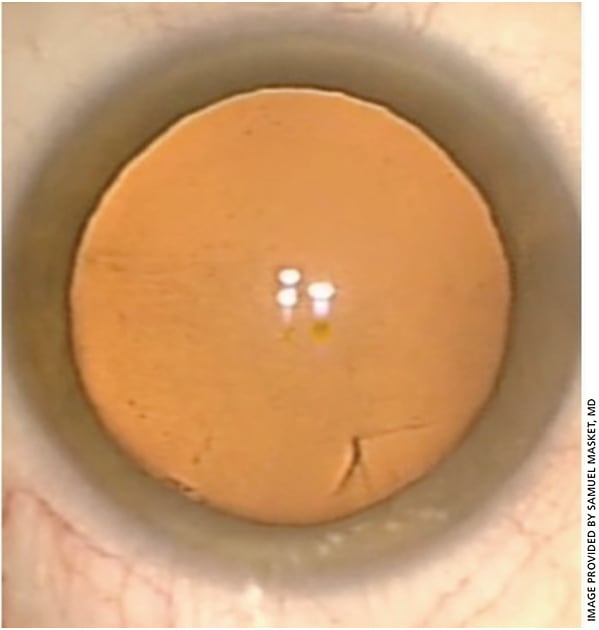
CASE #2: POSTERIOR POLAR CATARACT
The Malyugin ring (MST) has transformed the way we perform small-pupil cataract surgery; however, in some cases it is simply not feasible to use this device, so we must resort to iris hooks. An example of this scenario involves a 38-year- old woman with a classic posterior polar cataract (Figure 2).

In this patient, there were parapolar changes around the opacity, which sometimes signifies a defect in the posterior capsule. I thought there was a very strong case for using a femtosecond laser. Due to her age, ultrasound was not necessary to remove the nucleus.
After removing the nucleus and before removing the phaco tip, I used a viscodispersive agent and then performed viscodissection of the epinucleus and cortex. The OVD was fed under the capsule in several places, the phaco tip still inside the eye to prevent chamber collapse in case of a potentially defective or already torn posterior capsule. I prefer to remove the peripheral cortex, leaving only the posterior plate in place; the posterior plate is typically the last thing I take off the capsule in case the opacity is acting as a “cork” in the open capsule. I find, however, that once you have worked in the chamber, it is extremely difficult to avoid the anterior capsule if you need to insert a pupil expansion device (as was needed in this case) such as the Malyugin ring. In my opinion, it is safer to use iris hooks than the ring in this situation.
This patient’s posterior capsule was intact, so as it happens, the extra maneuvers weren’t necessary. Since the capsule can be as thin as 3 microns, I always use the technique in any patient with a posterior polar capsule, even if I don’t suspect a pre-existing defect. Also, while I don’t polish the posterior capsule, I do clean up the anterior capsule lens epithelial cells without any hesitation and urge others to do the same.
CASE #3: INDUSTRIAL INJURY
Twenty years ago, this patient had an industrial accident which perforated the limbus at the 4 o’clock position. The result was that his pupil was pulled down into this area. Despite this, he had been very active and was happy with his life, until a central nuclear cataract increased glare and decreased his visual function.
The patient’s pupil was eccentric, did not have an intact sphincter and was not adequate in size; thus, it was not possible to use a Malyugin ring to expand the pupil as it was not technically feasible. Instead, I used iris hooks. In performing the capsulotomy I discerned that the zonule was strong so I did not anticipate any further zonulysis during surgery. I extensively cleaned the lens epithelial cells to prevent postoperative capsular contraction. It helps to have a clear view when you are doing this; again, the iris hooks were useful in this situation.
As I planned a permanent pupilloplasty, I thought it best to place a capsular tension ring should late zonulysis occur. I used 23-g Ahmed micro-tying forceps and a 10-0 polyester suture to close the pupil and to centralize it. Interestingly, the patient tolerated an eccentric pupil inferotemporally for a long time in the phakic state and because of the size of the lens there was no problem; however in the pseudophakic state an eccentric pupil would not be well tolerated.
Using microforceps and microscissors, I tied and cut the sutures to close down the iris defect. However, this created a pupil that was not normal in shape, so it became necessary to sculpt the pupil, using a vitrector to nibble away at the sphincter to make a small, round central pupil. The patient had normal postoperative vision.
FINAL CONSIDERATIONS
Microsurgical instruments and other innovative devices have enabled anterior segment surgeons to gain exquisite control in managing the difficult cases, whether dealing with small pupils, compromised zonular fibers, unusual capsule problems or iris defects. OM
About the Author
