







One in every four visits to the eye doctor is for dry eye disease, making it one of the most common reason for seeking care.1 For ophthalmologists not specializing in anterior segment, it is important to have a basic understanding of recent changes in the dry eye landscape. In the 1997 original edition of the textbook Cornea, it was stated, “The mechanism for lacrimal gland dysfunction in this condition is unclear.”2 Just 20 years later, the Tear Film Ocular Surface/Dry Eye WorkShop II study defined dry eye as “a multifactorial disease of the ocular surface characterized by a loss of homeostasis of the tear film accompanied by ocular symptoms in which tear film instability and hyper-osmolarity, ocular surface inflammation and damage and neurosensory abnormalities play etiologic roles.”3 The old concept of a three-layer tear film has changed to two layers: a basal mucin-aqueous mixture and an upper oily layer. “Pain without stain” may imply a neurologic component, hyperalgesia, in a small subset of very symptomatic patients.
Another factor in DED is meibomian gland disease (MGD), which, in an often-quoted study by Lemp et al,4 was involved in 86% of dry eye patients. In my experience, this percentage is likely even higher, as it is rare to see normal meibomian secretions in any patient over 40. In most cases, tear quality rather than quantity is the more important issue to recognize and treat.
Despite the plethora of patients seeking dry eye relief, many eye-care professionals have little interest in dry eye, partly due to a historical paucity of effective treatments — that has certainly changed. Although care for these patients is still dismissed by some practitioners, others have promoted dry eye centers of excellence. Accurate diagnosis and management is a win/win endeavor for doctors and patients.
Impaired focusing power
The air-tear film interface is responsible for two-thirds of the eye’s focusing power; significant light scattering (measured by HD Analyzer [Visiometrics]) in patients with dryness and punctate keratitis contributes to fluctuating and blurry vision, analogous to looking through a golf ball instead of a billiard ball. Up to 77% of pre-op cataract patients have dry eye (corneal staining).5
A treatment tune-up for this group is mandatory to meet high expectations, especially for premium IOLs. Not to be forgotten is the contribution of other preservative-containing eye medications such as chronic glaucoma drops. Some centers are recommending first-line treatment procedures such as thermal pulsation or intense pulsed light (IPL). Though helpful, these are certainly more pricey options and should not bypass basic treatments.
Meibomian gland disease
MGD is a terminal duct obstruction, either quantitative or qualitative, with changes in glandular secretion that can be either hyposecretory or hypersecretory. This interrupts the dispersal of glandular lipids into the tear film, which normally promote stability and delay evaporation.6 MGD is consistent with the tell-tale signs of evaporative dry eye disease, such as rapid tear break-up time, lid thickening, marginal telangiectasias and saponification (foamy margins). Simple meibomian gland expression with two cotton tip applicators can provide another indicator: oil gland quality. Patients with MGD yield creamy or toothpaste-like material, opaque meibum with keratinized cellular debris.
Another method is meibography, a dynamic transillumination technique that gives a visual image and often enhances patient understanding and compliance. Although the exact etiology has not been elucidated, oil gland dysfunction and bacterial overgrowth likely contribute to MGD and the subsequent tear film instability and inflammation. There is also NO-MGD, or non-obvious MGD, in which a normal anterior lid exam masks the hidden posterior meibomian gland obstruction.
Treatment options
Most treatment plans start with artificial tears. Several excellent non-preserved oil-containing tears are available, including Retaine (OCuSOFT), SootheXP (Bausch + Lomb), Refresh Optive Advanced (Allergan) and Systane Complete and Balance (Alcon).
Directed heat to the inner aspect of the lids combined with massage are the essential elements of thermal pulsation or LipifFow (J&J Vision). For those seeking a more convenient and cost-effective route, a microwavable reusable heat pack (i.e., Bruder Moist Heat Eye Compress, Oasis Rest & Relief or Bausch + Lomb Thera-Pearl Eye Mask) is an affordable hygienic option which, if habitually used twice daily, can be a good first approach. DiPascuale et al reported significant improvement in all 17 of their study’s post-LASIK dry eye patients, using one treatment: heat to the eyelids for 10 minutes, four times daily for one month.7 For more severe cases, moist heat at a controlled optimal temperature for up to 20 minutes may be used (TranquilEyes, Eyeeco). Moisture chamber goggles and night masks can also help.
Lid cleansing follows right after heat — think of it as a “1-2” process. Cleansing is important as bacterial load is reportedly 15 times greater in blepharitis patients than in healthy eyes.8 In 1985, washing the eye with baby shampoo was a state-of-the-art treatment; unfortunately, this “treatment” does not kill bacteria and actually removes helpful skin oils. We have evolved since then, and several excellent options are now available, including Avenova (NovaBay), Cliradex (Bio-Tissue), Oasis Lid & Lash (Oasis) and Zocuwipe (Zocular), to name a few. Some of these effectively treat Demodex-face mites that are especially fond of the upper eyelash bases. This is also commonly referred to as cylindrical dandruff.
A systemic macrolide antibiotic, i.e., low-dose doxycycline, is a time-honored blepharitis treatment because of both its antibiotic and anti-inflammatory properties. A viable alternative is topical Azasite (Akorn), which is azithromycin plus Durasite. This topical solution is used off-label on the eyelids and recently became more affordable. The vehicle vastly improves antibiotic performance as it becomes bactericidal instead of bacteriostatic and enhances persistence in the tissue. After a tissue-loading dose, a therapeutic level may last up to seven days. The old standby, bacitracin, still has excellent gram-positive coverage. Finally, for chronic use, erythromycin can be quite helpful.
Omega-3 deficiency, nearly ubiquitous in the population, is easily measured by a simple finger stick blood test.9 Several years ago at the ASCRS meeting, Frank Bucci, MD, discussed the benefits of Omega-3 essential fatty acids in dry eye treatment. He stressed the importance of the re-esterified triglyceride form for maximal absorption with minimal side effects. Subsequently, Greg Smith, MD, noted statistically significant reduction in corneal staining, improved tear breakup time and 100% symptomatic reduction in a group of 20 patients treated for eight weeks with 2.24 grams of re-esterified triglyceride Omega-3.10 A landmark study by Epitropoulos et al showed improvement in five different measured parameters, including tear osmolarity and tear breakup time.11 This research demonstrates the effectiveness of a treatment regimen that includes high-quality Omega-3 acids from a marine source (not plants). My treatment protocol follows this data, and I use the same product, PRN’s Dry Eye Omega Benefits, that was utilized in the study.
In true aqueous deficiency, tear volume is low, osmolarity is often high (greater than 308 mOsmol/L) and InflammaDry (Quidel) may be positive, indicating the presence of MMP-9. A short tapering course of loteprednol 0.5%, a steroid soft on side effects but not potency, quiets inflammation. It is the only ophthalmic corticosteroid with an on-label indication for superficial punctate keratitis. The addition of either Restasis (cyclosporine ophthalmic emulsion, Allergan) 0.05% or Xiidra (lifitegrast ophthalmic solution, Shire) 5% follows. Restasis’ 15-plus year track record demonstrates increased tear secretion and enhanced goblet cell (mucin production) function (191% in pre-approval clinical studies).12 Xiidra is the sole agent approved for signs (punctate keratitis) and symptoms (OSDI scores) of dry eye, and, in clinical trials, about 50% of patients felt improvement as soon as two weeks.13 Most patients can benefit from at least one of these two prescription medications. Unfortunately, the choice often comes down to insurance coverage. Punctal plugs should be used only after the tear film improves to avoid increasing toxic tears in an untreated dry eye.
A sample treatment plan
Any dry eye treatment plan that does not address MGD is deficient. Most of these patients have already failed artificial tears alone or are referred for significant morbidity. My approach is to start with several treatments, taper with improvement but continue some indefinitely. A typical plan for moderate MGD is hot packs twice a day for five to 10 minutes followed by lid hygiene, antibiotic drop to the margins at bedtime for two weeks then one to two times per week, lipid-containing tears four times daily and re-esterified triglyceride Omega-3 essential fatty acids.
A follow-up visit in two to three months shows improvement in most patients. Those who do not show improvement may have Sjögren’s syndrome, obliterated meibomian glands or another diagnosis. For the majority who do well, I recommend continued maintenance of daily lid hygiene, tears as needed and Omega-3s.
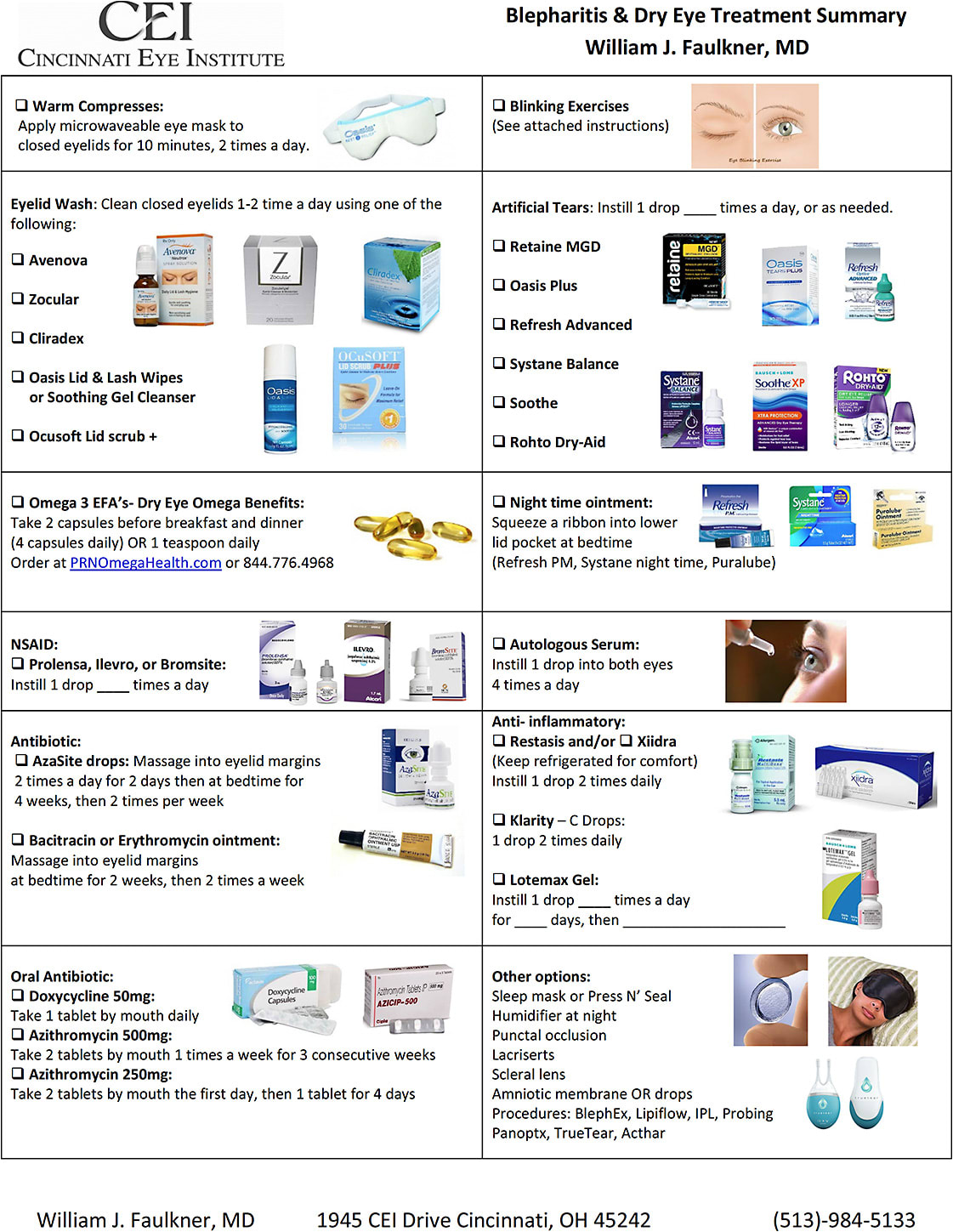
For patients with more severe or "plus" disease, alternative and additional choices are selected and highlighted on our treatment sheet:
Conclusion
Our privilege as physicians is to welcome, engage and connect with our patients. The hope is that if we are credible, personal and logical, they will trust us with their precious eyesight. Our duty is to first take an uninterrupted history, then use our knowledge and skill to make a diagnosis and agree on a plan in their best interest. I explain everything personally using visual aids, discuss research and articles, answer any questions and ask my assistant to reinforce all information. The recommended treatments above are highlighted on our handout, and additional relevant pamphlets are provided. OM

References
- Murphy, John J. Dry eye and inflammation: A discussion with Dr. Michael Lemp. MDLinx. http://bit.ly/2K3is9Y . Accessed June 1, 2018.
- Cornea, Vol II, Krachmer, Mannis, Holland. 1997 pg. 647
- Sullivan, DA. Et al. Conclusions and recommendations from the TFOS Dry Eye workshop II. July, 2017
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort: a retrospective study. Cornea 31:472-478.
- Trattler WB, Majmudar PA, Donnenfeld ED, et al. The Prospective Health Assessment of Cataract Patients’ Ocular Surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423-1430. Doi: 10.2147/OPTH.S120159.
- Nichols KK, Foulks GN, Bron AJ, et al. The International Workshop on Meibomian Gland Dysfunction: Executive Summary. Invest Ophthalmol Vis Sci. 2011, 52:1922-1929.
- DiPascuale MA, Liu TS, Trattler W, Tseng SC. Lipid Tear deficiency in persistent dry eye after laser in situ keratomileusis and treatment results of new eye-warming device. J Cat Refr Surg, 31, Sept. 2005.
- Bezza Benkaouha I, Le Brun C, Pisell PJ, Chandenier J, Lanotte P. (Bacterial flora in blepharitis). J Fr Ophthalmol. 2015:38:723-728. (French with English abstract)
- Omega Quant, Sioux Falls, SD
- Smith G, et al., Abstract Investigational Study, March, 2011 (Cornea Society Conference)
- Epitropoulos AT, Donnenfeld ED, Shah ZA, Holland EJ, Gross M, Faulkner WJ, Matossian C, Lane SS, Toyos M, Bucci FA, Perry, HD. Effect of Oral Re-Esterified Omega-3 Nutritional Supplementation on Dry Eyes. Cornea 35:9, Sept. 2016, 1185-1191.
- Proprietary information; Allergan. Irvine, CA.
- Proprietary information; Shire US Inc. Lexington, MA.