







The aging U.S. population has already started to result in more anterior segment surgeons seeing even more patients with visually significant cataract. As the baby boomer generation heads into “cataract age,” surgeons will likely see an increased numbers of patients with comorbidities they had not treated as much in years past. When patients with both cataract and glaucoma have yet an additional issue (corneal decompensation or a damaged iris, for example), determining which procedure to use and in what order to schedule them relies on a combination of surgeon and patient preferences as well as ease of procedure.
Three veteran specialists offer their pearls on dealing with these complicated cases.
PHACO-MIGS
Before you jump in
In recent years, the introduction of multiple microinvasive glaucoma surgery (MIGS) devices that are approved for use with concurrent cataract surgery has increased the number of phaco-glaucoma procedures.
Any patient who has cataract and glaucoma should be considered for MIGS regardless of how well controlled (or not) the glaucoma is, according to Michael Greenwood, MD, of Vance Thompson Vision in Sioux Falls, S.D. When MIGS was first introduced, “a lot of surgeons” were concerned they could not offer sufficient pressure-lowering control in people with elevated baseline pressures, he says. But, as the number of patients implanted with these devices increases, surgeons are finding they are capable of lowering pressures by as much as 7 mm Hg.
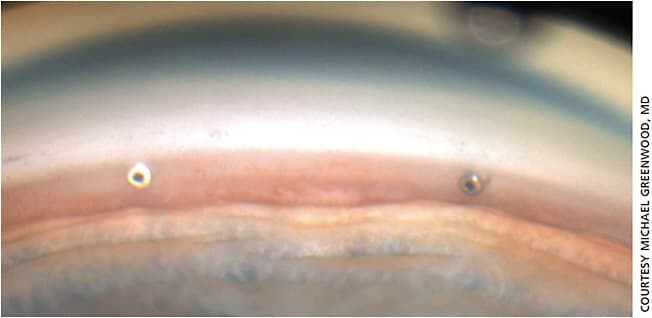
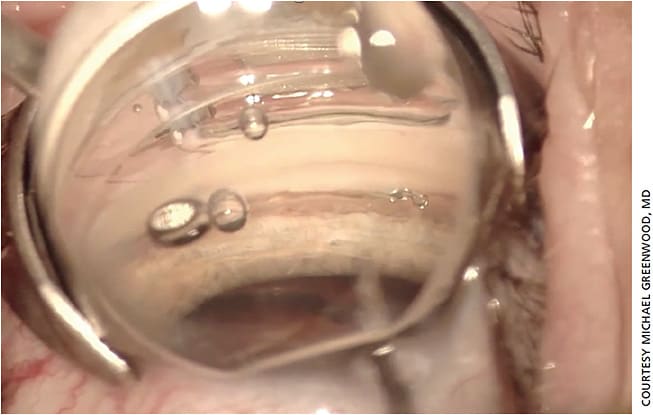
“For someone who’s just starting with the newer MIGS devices, the overarching piece of advice is to use whatever technology works best in your hands,” says Dr. Greenwood. “That’s what is going to be best for your patients, whether it’s the iStent (Glaukos) (Figure 1), the Hydrus (Ivantis) (Figure 2) or the Kahook Dual Blade (New World Medical).”
He recommends “familiarizing yourself with the angle anatomy before fully incorporating MIGS into your practice,” reaching out to surgeons and attending wet labs or conferences to get hands-on training.
Cataract surgery alone is well known to lower pressures; the advantage of adding a MIGS device is that “you’ll still have room to do something more later on, whether it’s an additional MIGS procedure or a filtering procedure, like a tube or a ‘trab,’” he says.
Patient selection
For some types of glaucoma, however, Dr. Greenwood does not recommend MIGS. Cases of chronic angle closure are one such example, “where there’s no view of the trabecular meshwork.” These may be better served by endocyclophotocoagulation or a conjunctival MIGS device (such as the XEN [Allergan]), he says. Patients with acute vascular glaucoma are another subset for whom MIGS may not be the best option.
“In more complicated cases, I recommend a stepwise approach,” he says.
Reimbursement issues
With MIGS devices, reimbursement can differ based on geographic location, Dr. Greenwood says. Surgeons need to understand what payments are for each particular code for each particular device (in some cases, simply performing the same surgery with the same staff and same device across a state border can result in doubled surgical reimbursements). On occasion, Dr. Greenwood has encountered situations in which the insurer will not pay for a MIGS procedure because the patient has not been prescribed a topical medication (even if the patient has visually significant cataracts).
PHACO-IRIS REPAIR
Before you jump in
Phakic patients are “a lot more challenging” when there is a concurrent need for iris repair, says Arsham Sheybani, MD, of Washington University School of Medicine in St. Louis, Mo. Often the cause of iris damage is trauma (if the trauma was nonpenetrating, or never required surgery, the full iris tissue may be there). Several scenarios can lead to iris repair surgery, including:
- congenital mydriasis or corectopia
- post-surgical issues that may be bothersome (eg, peripheral iridectomy)
- herpetic eye disease
Herpetic eye disease is a rare cause, but it can cause necrosis of the iris or ischemia.
Sometimes the damage causes the iris to roll onto itself, where it starts to contract.
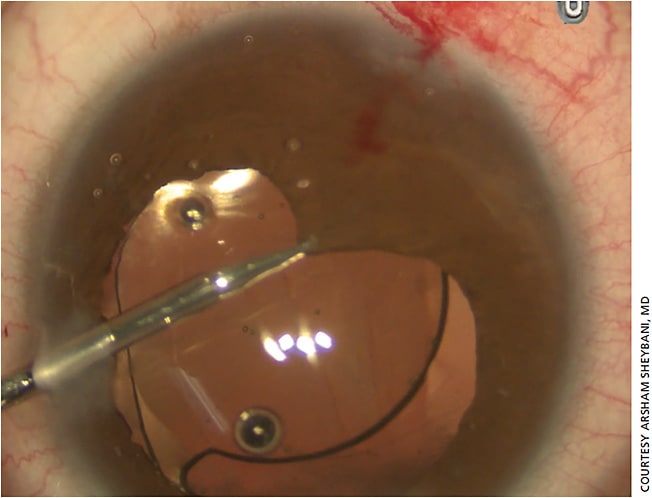
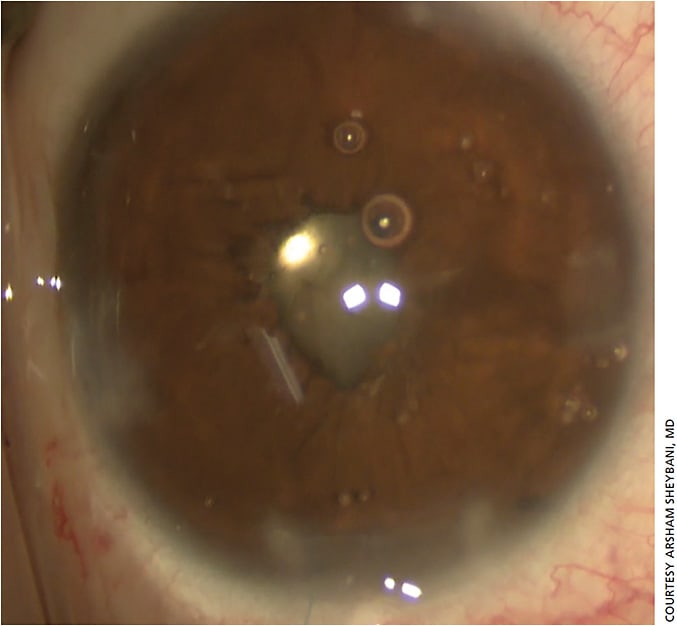
“The issue then becomes, how much tissue is there? If the iris was operated on before and the patient lost tissue, it’s a very different discussion,” Dr. Sheybani says (Figure 3).
Patient selection
When patients with glaucoma need both cataract surgery and an iris repair, the primary point to consider is whether or not the patient is bothered by the iris, Dr. Sheybani says. Surgeons should ask themselves, “Is the patient symptomatic? Is there light sensitivity or severe glare? Is there a cosmetic issue more so than an anatomic issue?” he says.
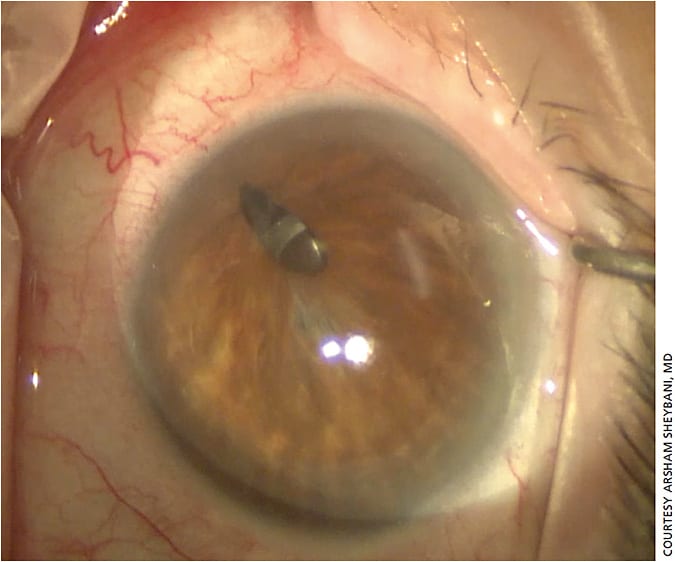
Asymptomatic patients are trickier, Dr. Sheybani notes. For example, in cases of corectopia, patients may end up with double vision because some light will go through the IOL while some may go around it only after cataract surgery is performed (Figure 4). But, suturing can sometimes cause more harm than good, he warns, especially if the iris is highly atrophic (Figure 5).
“In those instances, I consider using a prosthetic iris segment,” he says, adding that several devices are not approved in the United States, so surgeons may need permission from an institutional review board before using them in surgery.
“Bring the patient into the conversation as soon as you think you might need that device,” Dr. Sheybani says. “You may need a second surgeon to clarify that the procedure is necessary.” Clinicians should also be aware that insurance companies may cover the OR process and the cataract procedure, but not the device.
“Patients need to know what their financial responsibilities may be before they head into the surgery,” he explains.
Surgical planning
When planning the surgery, Dr. Sheybani recommends doing the cataract extraction and IOL implantation first, then moving onto the iris repair.
Preoperatively, knowing the pupil size of the contralateral eye in both light and dark conditions will help not only in choosing the appropriate IOL but also in counseling the patient about postoperative cosmetic differences between the two eyes.
Repairing a damaged iris at the time of cataract surgery “is not very cut and dried,” Dr. Sheybani explains.
Dr. Sheybani says knowing how thin an iris is (via color) can help to counsel patients about postop outcomes. Thinner irises may have glare or light sensitivity post-suture, whereas darker irises are less likely to.
When suturing, Dr. Sheybani prefers the channel Prolene on a CIF-4 needle (although the PC-7 is similar, he says). “It’s OK to make multiple corneal incisions. You want to plan out paracentesis incisions to make suture passes easier,” he says. “Postoperatively, the patient may need a longer course of steroids.”
Though it’s typical to have pigmentation continue to shed, he does not keep patients on steroids for shedding when checking the postop recovery. “But, if there are still white blood cells, then I would continue to use steroids. You want to be cognizant of how long you’re keeping patients on steroids,” Dr. Sheybani explains.
While not an ideal situation, phaco and iris repair can be managed successfully — but it takes more planning on the part of the surgeon.
PHACO-EK
Before you jump in
Combining endothelial keratoplasty (EK) procedures with phacoemulsification in patients with glaucoma may seem overwhelming and daunting, but using a MIGS devices, standard IOLs and Descemet’s membrane EK (DMEK) was shown by Stephens et al. at ASCRS this year to be safe and effective in patients with Fuch’s dystrophy.
For patients who are well-controlled on topical medications but also have mild Fuch’s dystrophy, “we’re going to be treating the cataracts and, if necessary, the Fuch’s dystrophy, and we can treat those simultaneously. Or, we’re going to treat them separately in either order,” says Evan D. Schoenberg, MD, Georgia Eye Partners in Atlanta, whose father also has mild Fuch’s and moderate cataract. “It’s a question of the balance of disease as well as the risk-benefit ratio for each procedure.”
Dr. Schoenberg says he typically views the glaucoma component as a separate entity in this subgroup of cataract patients, where the cataract and corneal disease are more crucial to address. Unless the corneal disease is highly advanced, patients are just as prone to dry eye issues as those without corneal issues, but Dr. Schoenberg prefers preservative-free glaucoma drops for these patients when possible.
Patient selection
For Dr. Schoenberg, a full exam and patient history is paramount to treatment decision-making. Patients with a moderate or worse cataract and mild Fuch’s should have the cataract addressed first, as “that patient may or may not actually need DMEK,” he says. Complaints of debilitating nighttime glare coupled with mild cataract and severe central guttae is indicative of the corneal issue, and the treatment plan should include DMEK.
Patient age makes a difference as well, Dr. Schoenberg says. “In patients who are 50 and older, I will almost always recommend the combined surgery, because we know that the cataract is likely to advance quickly after exposure to the air bubble that’s used to attach the DMEK graft, which means a guaranteed second surgery,” he says. “In a patient who’s younger than 50 where the cornea is the predominant problem, I’ll usually err towards doing just the DMEK initially and leave the lens alone, because that patient is more likely to be satisfied once the cornea is clear.”
Dr. Schoenberg says some cases warrant surgical treatment of Fuch’s first, even in cases of visually significant cataract.
“When there are severe epithelial bullae or corneal decompensation and significant cataract, I will treat the Fuch’s first, because I want to be able to acquire a better and more ‘normal’ keratometry reading to ensure I select the right IOL,” he says. The exception would be “if the cataract is so mature that its extraction is likely to require excessive phaco energy, which could damage the DMEK graft.” For that patient, combination surgery is most appropriate, along with counseling as to the possible variable refractive outcomes.
Surgical timing
Dr. Schoenberg contrasted his father’s case (who is well controlled on two drops, has mild Fuch’s, mild to moderate cataracts and has not had previous glaucoma surgery) to a 65-year-old patient with 3+ guttae, early corneal edema and an endothelial cell count of about 850 who recently had a XEN gel stent implanted but now presents with 3+ NS cataract in that same eye.
If “we’ve determined the patient needs simultaneous EK and cataract surgery and has already had filtering surgery, is it a DMEK or a Descemet’s stripping automated EK (DSAEK)? Would this patient benefit from just one of those procedures?” he asks. “If it’s the same patient without the active filtering surgery, without hesitation I would recommend simultaneous DMEK and cataract, because you’re not going to get the full benefit of surgery unless you treat both these problems.”
Not every patient is a candidate for DMEK, he says. In the above scenario, for example, he would perform phaco first, because he is concerned “about the challenges of getting any EK graft to adhere with a very recent filtering surgery. Air is going to escape the anterior chamber quickly. DMEK is going to be a big challenge, DSAEK less so because you don’t need as much air fill for DSAEK. If we can temporize with the cataract surgery alone and let the recent filtering surgery stabilize, the odds of initial success with EK are greater.”
Timing of previous surgeries should be another consideration, Dr. Schoenberg says.
“We know that the survival of the EK graft in the face of any filtering surgery is substantially lower than in a nonglaucomatous eye that has never had surgery,” he says. “If we can achieve good enough vision with cataract surgery alone and push the transplant into the future, that can be worthwhile.”
Luckily, Dr. Schoenberg says he’s never had an insurance company reject a claim because it believed a different order of surgery was indicated.
“There’s not this 30,000-foot view of a patient’s overall care plan from an insurance perspective; they’re generally dealing with it on a claim-by-claim basis,” he says. “Good documentation is important for insurance, for medical/legal and for patient counseling.” OM