







This fixed-dose combo is the second FDA approval for Aerie Pharmaceuticals’ Rho kinase (ROCK) inhibitor.
In March, the FDA approved Rocklatan (Aerie Pharmaceuticals), a once-daily drop containing the Rho kinase (ROCK) inhibitor netarsudil (0.02%) plus the prostaglandin analog latanoprost (0.005%) to reduce elevated IOP in patients with open-angle glaucoma or ocular hypertension. The company’s first-in-class netarsudil product, Rhopressa, received FDA approval about a year ago. Data from a pair of late-stage clinical trials show that Rocklatan lowers IOP more effectively than either of its components. Rocklatan is the first agent to demonstrate superiority to latanoprost in Phase 3 trials.1-3
Chairman and CEO of Aerie Vicente Anido Jr., PhD, recognizes the company’s unique position with these two offerings. “Together, Rocklatan and Rhopressa give us a broad therapeutic franchise, based on our ROCK inhibitor netarsudil, that addresses many of the needs of clinicians and patients in a wide variety of treatment settings,” he says.
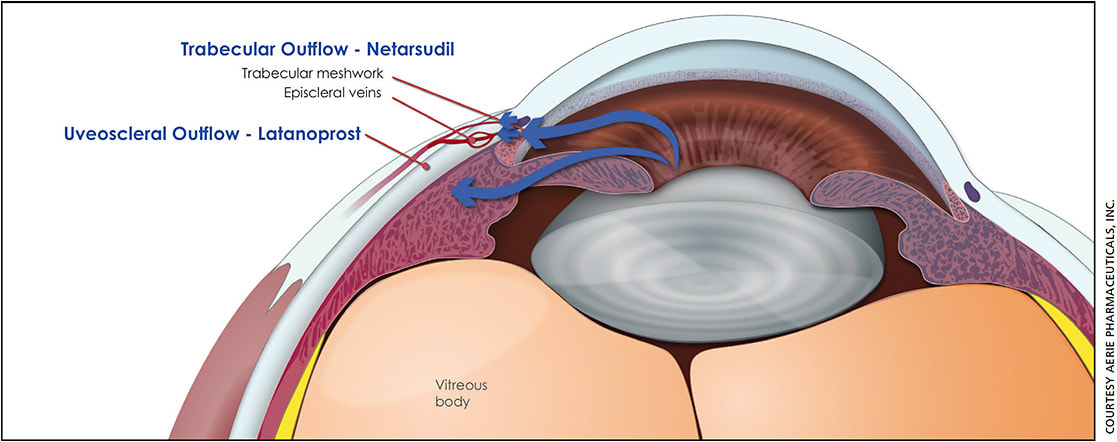
The ROCK inhibitor was specifically designed to target diseased trabecular meshwork (TM), the main cause of elevated IOP in open-angle glaucoma and ocular hypertension. Rhopressa works by restoring outflow through the TM, unlike latanoprost, which increases fluid outflow through the uveoscleral pathway.
APPROVAL DATA
Aerie’s multicenter Phase 3 trials, MERCURY 1 (12-month study) and MERCURY 2 (three-month study), randomized patients with open-angle glaucoma or ocular hypertension to receive Rocklatan, netarsudil or latanoprost.2 In both studies, Rocklatan achieved its primary 90-day efficacy endpoint, demonstrating superior IOP reduction over latanoprost and netarsudil at every time point. More than 60% of patients taking Rocklatan achieved an IOP reduction of 30% or more, nearly twice that achieved by latanoprost alone. Additionally, compared with the latanoprost arm, nearly twice as many patients in the Rocklatan arm reached an IOP of 16 mm Hg or lower and nearly three times as many reached 14 mm Hg.3
The majority of ocular adverse events (AEs) were mild and tolerable in the controlled clinical studies with Rocklatan. The most common, reported in 59% of patients, was conjunctival hyperemia. Notably, nearly 20% of patients had hyperemia at baseline, more than 90% of patients who experienced conjunctival hyperemia reported it as mild, the severity did not increase over time and 5% of patients discontinued due to the issue. Other common ocular AEs reported include instillation site pain (20%), corneal verticillata (15%) and conjunctival hemorrhage (11%).
IN CLINICAL PRACTICE
“There are three immediate advantages to Rocklatan for patients: simplifying drug regimens, enhancing compliance and decreasing copayments,” says Ruth Williams, MD.
The importance of simplifying drug regimens for glaucoma patients cannot be overstated, as specialists lament the depressing statistics around adherence to therapy. “When patients respond to a prostaglandin analogue and netarsudil, the combination agent is an obvious choice,” says Dr. Williams, who is a glaucoma consultant at the Wheaton Eye Clinic in Illinois and vice chair of the Glaucoma Research Foundation.
The netarsudil-based products are often particularly effective in patients who have good pressures but require even lower numbers, Dr. Williams says. “For patients with pressures in the mid-to-low teens already, it is usually difficult to lower the pressure even more. With Rocklatan, several patients now have pressures in the single digits.”
This effect is likely due to its lowering of episcleral venous pressure, she adds. ROCK inhibitors target the TM at the subcellular level, binding to the protein Rho kinase, or ROCK. This disrupts the interaction of myosin with actin, causing disassembly of actin stress fibers and anchoring complexes, thereby relaxing the TM.4
“We have been waiting for a new drug with a unique mechanism of action for a long time, so Rocklatan and Rhopressa are exciting additions. In patients with severe glaucoma who require a low target pressure or for normal tension glaucoma patients in need of a ‘lower number,’ I often prescribe the recently approved combination,” Dr. Williams says.
“We have also been working diligently on securing favorable reimbursement for our products,” adds Dr. Anido, “with Rhopressa now enjoying broad commercial and Medicare Part D coverage, and Rocklatan already under review by major payers.”
SIDE EFFECT DISCUSSIONS
Dr. Williams notes that her clinical experience does reflect that of the clinical trial — red eye can be a limiting factor. “It is important to set patients expectations with regard to this outcome,” she says. “Therefore, I tell my patients upfront that about half of the patients get redness when starting the drop and that some patients have to discontinue use.”
Dr. Williams accepts that this discussion is part of the journey and that, sadly, no drug is perfect. “I tell patients that I think it is worth the trade off because netarsudil can sometimes be so effective. Ultimately, patients can weigh the benefits of an effective drug with the side effects and determine if it is worth it for them.”
CONCLUSION
Aerie is positioning Rocklatan as first replacement for PGA monotherapy and has launched it at a small price premium to Rhopressa.
The new agent is the only fixed-dose combination containing a prostaglandin analog approved in the United States and the only combination glaucoma drug administered once daily. OM
Disclosure: Dr. Williams is a consultant to Aerie.
REFERENCES
- Rocklatan (netarsudil and latanoprost ophthalmic solution) 0.02%/0.005% Prescribing Information, Aerie Pharmaceuticals, Inc., Irvine, Calif. 2019.
- Asrani S, McKee H, Scott B, et al. Pooled phase 3 efficacy analysis of a once-daily fixed-dose combination of netarsudil 0.02% and latanoprost 0.005% in ocular hypertension and open-angle glaucoma. Presented at the 13th Biennial Meeting of the European Glaucoma Society, March 2018.
- Data on file, Aerie Pharmaceuticals, Inc.
- Wang SK, Chang RT. An emerging treatment option for glaucoma: Rho kinase inhibitors. Clin Ophthalmol. 2014;8:883-890.