







NATHAN M. RADCLIFFE, MD (moderator): The recently published results of the LiGHT (Laser in Glaucoma and ocular HyperTension) trial, and the ensuing role of SLT in the glaucoma treatment paradigm, are the most significant news in glaucoma treatment to emerge this year.1 Dr. Craven, would you please describe the LiGHT trial and its findings?
E. RANDY CRAVEN, MD, FACS: The LiGHT trial was an observer-masked, randomized, controlled clinical trial in which more than 700 patients newly diagnosed with open-angle glaucoma or ocular hypertension were randomized to receive either selective laser trabeculoplasty (SLT) as initial treatment or intraocular pressure (IOP)-lowering eye drops (often latanoprost) as initial treatment. Patients were enrolled from six hospitals across the United Kingdom. They weren’t eligible if they had undergone previous intraocular surgery, unless the surgery was uncomplicated phacoemulsification received at least 1 year prior to randomization. Patients with exfoliative glaucoma and pigmentary glaucoma were included.
The LiGHT trial differed from some previous laser trials in that patients, not eyes, were the unit of analysis. When a patient had both eyes in the study, baseline severity and IOP were based on the worse eye. Target IOP was set for each patient according to glaucoma severity. For setting target IOP, investigators used the consensus guidelines developed by Karim Damji and researchers across Canada.2 As such, up to a 30% reduction in IOP was sought.
For the SLT group, the treatment was delivered to 360 degrees of the trabecular meshwork using 100 non-overlapping spots at energy levels of 0.3 to 1.4 mJ. This is relatively low energy, and the average energy used was less than 1 mJ. Repeat SLT was permitted, and SLT could be followed by medication, if required.
For the eye drops group, investigators used a predetermined pattern for medication choice. Patients were started on a prostaglandin analog. If a prostaglandin analog wasn’t an option or wasn’t effective, a beta blocker was the next choice. If additional medication was needed, either a carbonic anhydrase inhibitor or an alpha agonist was used.
Patients were followed for 3 years, and the primary outcome of the trial was health-related quality of life (HRQoL) based on multiple questionnaires. Secondary outcomes included cost-effectiveness, clinical effectiveness, and safety. According to the results, SLT as first-line therapy costs less and provides the same degree of efficacy with regard to clinical outcomes and HRQoL (Figure 1).
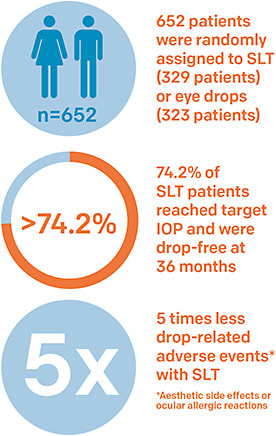
Remarkably, 74.2% of the patients for whom SLT was the initial therapy didn’t require the addition of medication to control IOP. Also, remarkably, the SLT patients were at their target IOP for 93% of their study visits. Zero patients in the SLT group required incisional surgery during the course of the study compared with 11 patients in the medication group. In my mind, this suggests SLT may be disease-modifying.
LiGHT Study Builds on Previous Research Findings
DR. RADCLIFFE: Though not mentioned in the LiGHT paper, the previous work of Mark Latina, MD, and L. Jay Katz, MD, has been instrumental in our understanding of SLT.
ROBERT J. NOECKER, MD, MBA: Yes, that perspective is important. I was one of the clinical investigators in the phase 3 FDA trials that evaluated SLT3 and also an investigator in the Katz (SLT/Med study) trial4 (Figure 2). In the late 1990s, while we were pursuing approval for SLT, the FDA only allowed us to have two SLT treatment groups: prior failed argon laser trabeculoplasty (ALT) and maximal medical therapy. We proposed a third group, SLT as primary therapy, which wasn’t allowed. Therefore, we were starting with an unfavorable patient population, which contrasts with the LiGHT trial. Nevertheless, we were able to show that SLT lowered IOP by 3 mmHg on average, an approximately 20% reduction, which we believed was significant given the patient population. And we showed SLT was safe.
| SLT | Medication | |
|---|---|---|
| Baseline IOP | 24.5 mm Hg | 24.7 mm Hg |
| Post-treatment IOP | 18.2 mm Hg | 17.7 mm Hg |
| The results of the LiGHT trial support the findings by Katz and colleagues, published in 2012, in which SLT was demonstrated to achieve the same IOP-lowering effects of medication when used as a first-line therapy.4 | ||
Originally, SLT was used similarly to ALT, mainly after medications had failed. But, as physicians became more comfortable with SLT, they began to use it earlier in the course of treatment. That brought us to the Katz trial in which patients were randomized to receive either SLT or medical therapy. This was a rigorous study with aggressive pressure-lowering goals. Patients in both groups achieved their target pressures (Figure 2) in the mid-teens at approximately the same rate — but, with SLT, it took fewer steps to reach that point.
Restoring Aqueous Outflow Via a Biologic Mechanism
DR. RADCLIFFE: Dr. Singh, please describe the mechanism of action of SLT. Also share your insights about restoring aqueous outflow through the conventional pathway, mechanical versus biological effect, and how all of this fits with minimally invasive glaucoma surgery (MIGS) and other types of treatments.
PAUL SINGH, MD: It’s important to keep in mind that we don’t know exactly where aqueous outflow encounters resistance in the conventional pathway. Resistance may be based in the trabecular meshwork, Schlemm’s canal, or distal collector channels. In patients with advanced disease who have been using multiple IOP-lowering drops for multiple years, damage may also have occurred distally to the trabecular meshwork. Therefore, it stands to reason that SLT or any type of trabeculoplasty is less likely to be as effective as it would be in patients with less advanced disease in whom more parts of the pathway may still be functioning. Earlier disease lends itself to a more optimized outcome.
When it comes to mechanism of action, SLT actually addresses the site of pathology rather than suppressing aqueous or diverting fluid away from the TM, as we do with many of our current drops. The mechanical theory of ALT works by causing thermal damage. With electron microscopy, we’ve seen the physical separation of the trabecular beams and the thermal damage adjacent to the separation that ALT causes. It’s a contracting and expanding type of mechanism.
Thermal burns to the trabecular meshwork cause tissue contraction and tightening of the trabecular ring. The tissue is opened and outflow increases — but with the negative effect of fibrosis in some areas of Schlemm’s canal. This works against the usefulness of MIGS, which requires a patent canal. The thermal damage levied by ALT is why I stopped using the procedure many years ago.
SLT, on the other hand, doesn’t cause thermal damage. SLT uses a Q‐Switched frequency‐doubled (532 nm) Nd:YAG laser, which selectively targets melanocytes in the pigmented trabecular meshwork. The architecture of the canal and the trabecular meshwork is maintained. The mechanism is mainly physiologic rather than mechanical. SLT utilizes the body’s natural reaction to release metalloproteinases, interleukins, and cytokines, which stretch and thin the beams of the trabecular meshwork to increase outflow. SLT is thought to be a selective photothermolysis. Because only the pigmented cells are targeted and there is no thermal damage, we do not see peripheral anterior synchiae. The pulse duration is shorter (3 nsec) than the thermal relaxation time of melanin (1 msec), which allows for less damage to the architecture of the TM.
SLT also uses lower energy than ALT. SLT classically uses around 1 mJ or less of energy, whereas ALT uses around 50 mJ (500 mW for 0.1 s). This makes the energy used by SLT 50 times lower than in ALT. Because the energy in ALT is aimed at an area 64 times smaller than in SLT, the energy per mm2 of tissue is 3520 times smaller in SLT than in ALT.
The body’s own reaction and release of these enzymes and modifying factors allow for a natural rejuvenation, so to speak, of the outflow system. Again, this physiologic approach maintains the potential for success of future procedures, such as MIGS, if they’re needed.
DR. NOECKER: I agree that the mechanism of SLT, as with all laser trabeculoplasty, is biologic rather than mechanical, and I consider ALT to be overtreatment. ALT creates burns — essentially, dead tissue. ALT may induce tissue contraction, which can help outflow but some viable trabecular tissue may be sacrificed. SLT induces long-term positive changes in the porosity of the Schlemm’s canal endothelium.
As Alvarado and colleagues showed, SLT creates low-level damage that releases leukotrienes and recruits monocytes and macrophages, which rejuvenate the outflow pathway.5,6 An initial chemical response produces the one-day post-procedure IOP decrease that we see, and it’s followed by the cells moving in and inducing long-term changes.
Another important point about the SLT mechanism of action is that treatment in one eye lowers IOP in the fellow eye, typically by a few mmHg,7 an effect we’ve all seen in practice. This supports that the mechanism of action is biologic.
It’s worth noting, too, that our histopathologic work showed SLT energy is absorbed by cells that contain pigment,8 and any trabecular cell in an eye that isn’t albino contains pigment. That’s why SLT works even in lightly pigmented eyes. Success doesn’t depend on needing significant pigment, as it did with ALT. That was the mantra doctors followed with ALT: You need more pigment, or it isn’t going to work.
SLT is a tool that allows us to also use other treatment options. I often use an aqueous suppressant with SLT. The combination of decreased aqueous production while improving outflow works very well.
DR. RADCLIFFE: I believe SLT will marry nicely with the newer medications, too. They’re described as trabecular outflow agents, but there is evidence that both latanoprostene bunod (Vyzulta, Bausch + Lomb) with its nitric oxide moiety and netarsudil (Rhopressa, Aerie Pharmaceuticals) lower episcleral venous pressure as well. If that’s the case, using them along with SLT will reduce outflow resistance at the level of the trabecular meshwork and also increase the drive to get the fluid out.
I’ve heard a concern that laser shouldn’t be used for patients who are on one of the next-generation medications, but I think it’s just the opposite. It’s probably a great opportunity.
DR. CRAVEN: I spoke with LiGHT trial lead investigator Gus Gazzard about this, and he said most of the people in the trial had relatively light irides, which shows amount of pigment isn’t an issue with SLT.
SLT Mitigates Medication-related Challenges
DR. RADCLIFFE: Relying on medications to control IOP saddles our patients and practices with multiple burdens that SLT can help to alleviate.
LARRY PATTERSON, MD: As a general ophthalmologist, I tend to see glaucoma patients earlier on the spectrum than a glaucoma specialist sees them. That typically means I have two options I can recommend: drops or laser. Drops introduce the issues of cost, compliance, and side effects. Cost can vary substantially. The newer drops can be expensive even with insurance. Although older medications can be less expensive, patients have to continue to pay for them for the rest of their lives.
As far as compliance, even a once-a-day drop is difficult to remember. Patients are tethered to the medications. Their lives revolve around using the drops. They also face the potential side effects — right now and in the long term. The “right-now” side effects are problems such as burning, stinging, and blurry vision. In the long term, preservatives in drops may lead to dry eye or conjunctival toxicity that can complicate trabeculectomy. We also suspect and have questions about whether drops damage the outflow pathway.
When I talk with colleagues about SLT, many say they don’t believe patients want laser as first-line treatment. In my opinion, that depends on how it is presented to them. I don’t necessarily try to persuade patients to choose laser instead of drops. I give them my honest assessment of the two options.
I briefly lay out the challenges associated with drops. I say it’s very important to use the drops to keep the eye pressure under control to prevent optic nerve damage, but drops have downsides. On the other hand, I tell patients that side effects are rare with the laser. And having insurance cover the cost of SLT will likely be more straightforward than it typically is with medications.
Most importantly, SLT is very likely to work. I also mention that by laser I don’t mean a laser that you’d see burning a hole through a steel vault in a James Bond movie. The SLT laser is extraordinarily low power — a very gentle beam of light that induces changes in the eye that will make the fluid flow out better.
DR. CRAVEN: I’ve seen a generational change in that younger people more and more are interested in minor procedures versus medications.
DR. SINGH: I agree we should present patients with their options, but I also think we should let them know what we think is best for them based on medical science. For me, based on my clinical experience and now the LiGHT study, there’s no doubt that SLT is the better option as a first-line treatment considering the numerous compliance issues with drop therapy. Therefore, I present it as “this is what I prefer for you.”
DR. NOECKER: I phrase it a little differently in my discussions with patients. I avoid being negative about drops; I like to keep the entire discussion positive. I explain that we treat glaucoma with both medication and lasers, and that’s the case for most of my patients.
DR. SINGH: I agree we should keep it positive for both laser and drops, but I do think if, as a provider, you think there are some specific benefits to SLT, it is important to highlight those benefits and explain the value to the patient.
I also like to use the phrase, “SLT is a beam of light that rejuvenates your natural drainage system.” This way, they don’t get turned off right away as compared with when I initially use the word “laser.”
DR. RADCLIFFE: When I think about the difference between telling patients SLT and medications are equivalent and telling them SLT is superior, I refer to my own “aha” moment. Mocan published a paper on meibomian gland dysfunction (MGD) in glaucoma patients utilizing IOP-lowering drops for more than 12 months.
An overwhelming majority of the patients who were using a prostaglandin analog had MGD, and a majority of patients using a drop that wasn’t a prostaglandin analog had MGD.9 We’re certainly aware of how widespread a problem dry eye is and how it interferes with cataract surgery outcomes. Why would we want to add fuel to that fire when in SLT we have a solution that takes it off the table?
DR. SINGH: Keeping patients happy and compliant is probably the most difficult issue I face with medical management of glaucoma. A report from Erb based on a database of 20,000 patients in Europe also showed the extent of dry eye in the glaucoma patient population, particularly when three or more medications were being used.10 This matters on several levels, including that patients tend to blame the drops when they have dry eye disease and, consequently, often stop using them or use them only periodically.
This is a serious problem, especially in more advanced disease. Data from the Advanced Glaucoma Intervention Study (AGIS) showed that IOP fluctuation is associated with visual field progression. Even patients with low mean IOP (10.8 mmHg) demonstrated the same risk of progression as those patients with high mean IOP (20.8 mmHg).11 So, if fluctuations occur at low pressure in more advanced disease, that alone can be a risk factor for progression. This is a major reason with regard to compliance that SLT is a good option.
LiGHT Trial Has Potential to Change Glaucoma Treatment Paradigm
DR. SINGH: With awareness of the LiGHT trial results, I believe the entire glaucoma treatment paradigm will change to a more interventional approach. Once more physicians and patients think of SLT — rather than medications — as the most desirable first-line treatment option, the choice of MIGS will be more frequent as well. Some people will still need drops, of course.
Drops can be the savior in some patient scenarios. However, SLT will come earlier in the disease process, perhaps combined with drops along the way, which will also bring MIGS front and center earlier. SLT as first-line treatment will foster change in the overall paradigm.
DR. CRAVEN: I think the LiGHT trial will change the conventional wisdom substantially.
DR. NOECKER: It surely will change the question from “Why use SLT as first-line therapy?” to “Why not use SLT as first-line therapy?”
DR. RADCLIFFE: If interventional glaucoma is the future of glaucoma care, SLT as primary therapy is definitely the first and easiest step to take in that direction.
Stabilizing IOP Fluctuations with SLT
DR. RADCLIFFE: What are the benefits of SLT in controlled glaucoma? In low-pressure glaucoma?
DR. RADCLIFFE: The fact that SLT keeps nocturnal IOP at bay is important. One of my greatest concerns about low-pressure glaucoma is that it’s essentially glaucoma that spikes at night.
Even if a patient’s IOP is the same before and after SLT, I suspect we’re measuring a fluctuation in the office and eliminating nighttime spikes. I like that I’m treating the patient with more than just drops.
DR. NOECKER: All of the studies show the higher the starting IOP, the bigger percentage IOP decrease SLT will produce. But, even if IOP is 10 mmHg, there’s room for improvement. As eyes age, outflow facility decreases. Over time, they lose the buffer against pressure fluctuations.
So, even when it appears the trabecular meshwork is working well based on our in-office IOP readings, as Dr. Radcliffe said, it’s probably not. With SLT, we can optimize the meshwork and help to stabilize pressure fluctuations. The Normal Tension Glaucoma Trial showed further lowering of low pressure is beneficial.12
Durability and Repeatability with SLT
DR. CRAVEN: I view SLT as part of an overall glaucoma treatment pattern. Is there a threshold number of treatments after which you’ll stop using it?
DR. NOECKER: For me, it’s patient-dependent. On average in my practice, the effect lasts 2 to 3 years, which is what most of the published studies show. However, I’ve had patients go as long as 7 years without further treatment. In my opinion, and there are studies to support this, if you get a good response the first time, it’s worth doing again. In other words, success predicts future success. I have treated one patient five times because it continued to work.
DR. PATTERSON: When you perform SLT and get a great response, how soon would you repeat it if IOP begins to come back up? I ask because, in my general ophthalmology practice, we perform a significant number of anti-VEGF injections for retinal disease. We see an IOP increase in approximately 2% or 3% of these patients and SLT works phenomenally well to bring it back down.
DR. NOECKER: It can be effective in steroid responders, too. To answer your question, I don’t hesitate to re-treat in 6 months, if necessary.
DR. SINGH: A study by Hong and colleagues showed the IOP-lowering effect of a second SLT treatment performed at least 6 months after an initial SLT treatment to be the same as achieved with the first treatment.13 In my experience, the earlier SLT is used, the longer the effect lasts. Also, repeat treatments tend to work better in patients whose disease is in the earlier stages. ●
References
- Gazzard G, Konstantakopoulou E, Garway-Heath D, et al.; LiGHT Trial Study Group. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial. Lancet. 2019;393(10180):1505-1516.
- Damji KF, Behki R, Wang L; Target IOP Workshop participants. Canadian perspectives in glaucoma management: setting target intraocular pressure range. Can J Ophthalmol. 2003;38(3):189-197.
- Latina MA, Sibayan SA, Shin DH, Noecker RJ, Marcellino G. Q-switched 532-nm Nd:YAG laser trabeculoplasty (selective laser trabeculoplasty): a multicenter, pilot, clinical study. Ophthalmology. 1998;105(11):2082-2090.
- Katz LJ, Steinmann WC, Kabir A, et al.; SLT/Med Study Group. Selective laser trabeculoplasty versus medical therapy as initial treatment of glaucoma: a prospective, randomized trial. J Glaucoma. 2012;21(7):460-468.
- Alvarado JA, Alvarado RG, Yeh RF, Franse-Carman L, Marcellino GR, Brownstein MJ. A new insight into the cellular regulation of aqueous outflow: how trabecular meshwork endothelial cells drive a mechanism that regulates the permeability of Schlemm’s canal endothelial cells. Br J Ophthalmol. 2005;89(11):1500-1505.
- Alvarado JA, Katz LJ, Trivedi S, Shifera AS. Monocyte modulation of aqueous outflow and recruitment to the trabecular meshwork following selective laser trabeculoplasty. Arch Ophthalmol. 2010;128(6):731-737.
- Rhodes KM, Weinstein R, Saltzmann RM, et al. Intraocular pressure reduction in the untreated fellow eye after selective laser trabeculoplasty. Curr Med Res Opin. 2009;25(3):787-796.
- Kramer TR, Noecker RJ. Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology. 2001;108(4):773-779.
- Mocan MC, Uzunosmanoglu E, Kocabeyoglu S, Karakaya J, Irkec M. The association of chronic topical prostaglandin analog use with meibomian gland dysfunction. J Glaucoma. 2016;25(9):770-774.
- Erb C, Gast U, Schremmer D. German register for glaucoma patients with dry eye. I. Basic outcome with respect to dry eye. Graefes Arch Clin Exp Ophthalmol. 2008;246(11):1593-1601.
- Caprioli J, Coleman AL. Intraocular pressure fluctuation a risk factor for visual field progression at low intraocular pressures in the advanced glaucoma intervention study. Ophthalmology. 2008;115(7):1123-1129.e3.
- Anderson DR; Normal Tension Glaucoma Study. Collaborative normal tension glaucoma study. Curr Opin Ophthalmol. 2003;14(2):86-90.
- Hong BK, Winer JC, Martone JF, Wand M, Altman B, Shields B. Repeat selective laser trabeculoplasty. J Glaucoma. 2009;18(3):180-183.