







Ask surgeons to rate their cataract and refractive surgery outcomes and, after reflecting on recent cases, they will usually conclude that they are doing pretty well. The problem with using memory recall as a method of tracking your outcomes is twofold: we tend to remember our successes better than our misses, and refractive outcomes require precise measurements to properly evaluate them.
In the quest for improved patient outcomes, surgeons often overlook tracking and optimization. Although it can be time consuming and requires analysis, examining and comparing outcomes can be extremely rewarding for surgeons. As the old adage goes, you never really know something until you study it. To become the best surgeon that you can be, you must actively analyze your surgical outcomes and use this as a platform for improvement.
In this day and age of big data, all surgeons have the tools to become experts on their own surgical practice. A number of commercial data management and analysis options are available that provide an easy entry point into outcomes tracking.
ONLINE
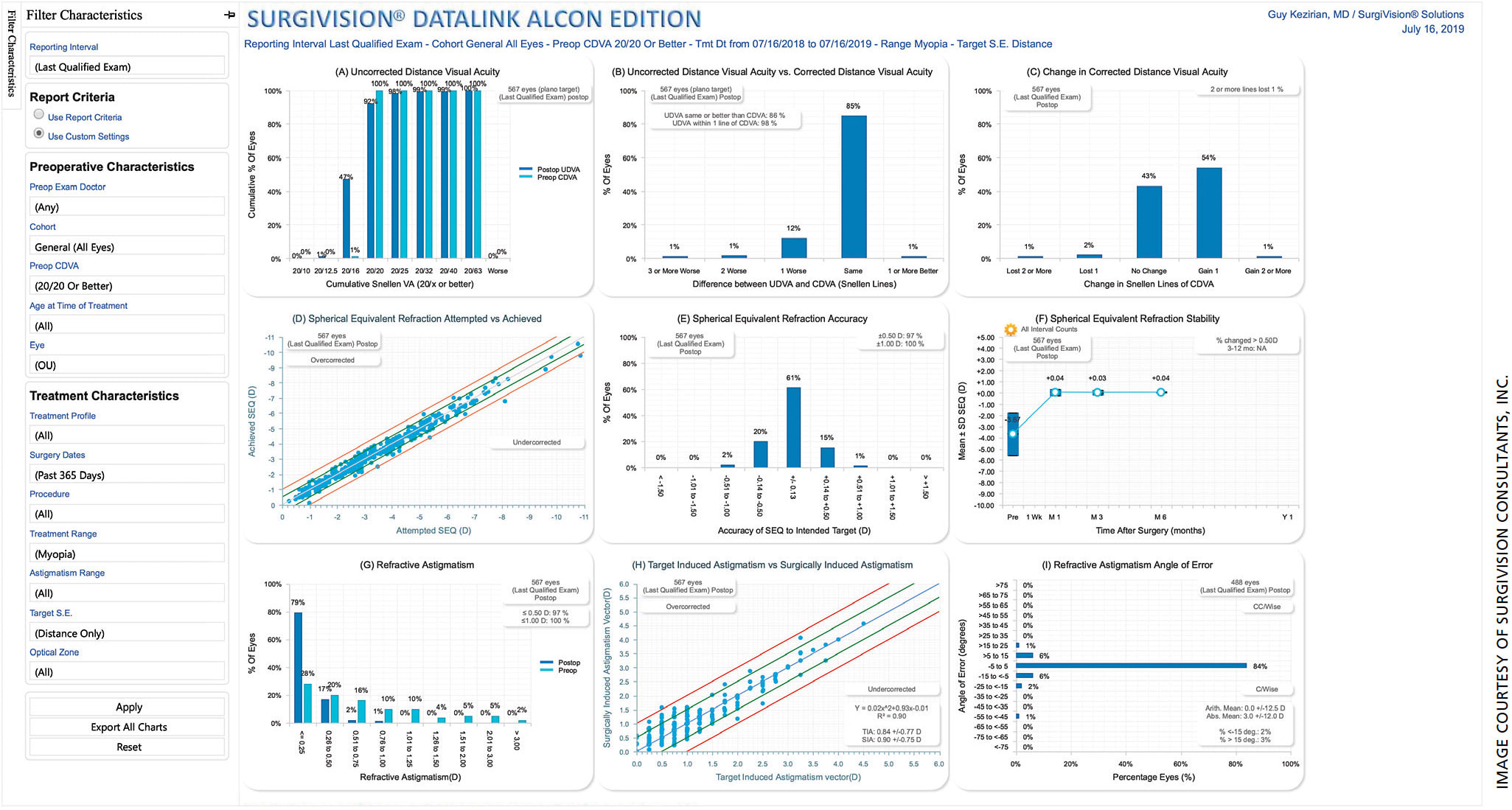
Several online data portals are commercially available. Perhaps the best established in the arena of laser vision correction is SurgiVision (www.surgivision.com ). Alcon, Johnson & Johnson Vision and Zeiss all participate in the SurgiVision DataLink portal for refractive outcomes tracking and nomogram adjustment. The service is free to use for surgeons (sponsored through industry support) and is an easy entry point into outcomes tracking. Based on outcomes that surgeons provide to the website, SurgiVision computes an updated nomogram. The more outcomes you enter, the better your nomogram gets (Figure). A refined nomogram results in more predictable and accurate refractive outcomes — and more happy patients.
BIOMETER SOFTWARE
Modern biometers offer a method of outcome tracking with included software to optimize lens constants used for IOL power calculations. Although this does not give surgeons an idea of how often they are hitting their refractive targets, a 2011 paper in the Journal of Cataract and Refractive Surgery by Aristodemou et al showed that iteratively optimizing lens constants improves refractive predictability. This is a worthwhile undertaking once a surgeon has accumulated 50 or more cases with a particular biometer and lens combination.
INTRAOPERATIVE ABERROMETRY
With the online portal for the ORA (AnalyzeOR), Alcon has included tools for users to track their outcomes and optimize the device. As surgeons enter postoperative refractive data from ORA cases, the portal dynamically analyzes the refractive outcomes to enhance the ORA system for future cases. It also provides the surgeon with handy reference data on postoperative outcomes, such as the average magnitude of cylinder decrease for toric IOL and astigmatic keratometry patients.
REGISTRY
Many larger institutions have begun to track outcomes through the use of registries, according to research from Qin et al published in 2018 in Current Opinion in Ophthalmology.
Although it has not yet started offering individual-level outcomes tracking, the AAO IRIS Registry offers an array of other services that can be beneficial for practitioners, including automated EMR integration with MIPS reporting, as noted by Parke et al in a 2017 paper in Ophthalmology. The use of this platform for individual physicians to track their own outcomes and compare them to the community has yet to be fully realized. This may develop into a useful tool for refractive cataract surgeons for outcomes tracking, but currently the system isn’t quite there yet.
MANUAL TRACKING
Although there are a number of commercial options available, physicians may manually track outcomes. Options include utilizing a reporting function from an EMR or manual entry in a spreadsheet.
Beginning this is as easy as starting a spreadsheet with columns for preoperative refraction, IOL type and power, intended target, IOL location (i.e., sulcus or bag), axis of position for toric IOLs and postoperative refraction. After 100 patients or so, look at your intended vs. achieved refraction. Break down your analysis by IOL type and patient status (i.e., postrefractive surgery, toric IOL or multifocal IOL).
Including more information, such as age, preoperative refraction or biometry, will give you more variables to analyze and track, but take care to avoid burdening yourself or your staff with too much information to record.
If you have an EMR, you can automate reports to do this for you. For example, at University of California, San Francisco, we are working with our IT department to create automatic outcomes reports using pre- and postoperative refraction data. Although establishing a manual tracking system requires more up-front effort, its utility can be long lasting.
CONCLUSION
Outcomes tracking is essential for optimizing the excellent refractive outcomes that today’s patients expect. Investing the time in setting up a system to measure and report your practice’s outcomes will lead to a better understanding of your surgical practice and improved patient care and outcomes. OM
About the Author
