







Intraocular pressure (IOP) is the most important modifiable risk factor in glaucoma. Typically, we look at peak pressure to calculate target IOP and develop a treatment plan, but this information often is missing. In fact, researchers have found that more than 75% of IOP measurements taken between 7 a.m. and 9 p.m. tend to miss the highest point of the diurnal curve.1 In other words, if we’re relying on single IOP readings taken in the office, we’re likely not capturing the potentially harmful pressure spikes that may lead to disease progression.2
To overcome this limitation, we believe it’s important to assess patients’ IOP over a longer period of time, not only at diagnosis but also before and after treatment. That’s where the iCare HOME2 tonometer comes into play.
Accurate, Reliable, User-Friendly
The iCare HOME2 tonometer applies the same rebound technology as the iCare tonometers we use in clinic, but it is designed specifically for patients to use at home throughout the day and night. The HOME2 is the next generation of the original iCare HOME, which we have used with great success in our practice, and it now incorporates new user-friendly features. For example, the iCare HOME2 provides visual and audio cues to help patients position the device properly for accurate measurements. Patients may use it while sitting, reclining, or in a supine position, which facilitates its use during the night and early morning hours.
This device provides a full picture of IOP fluctuations over time, enabling us to identify patterns, trends, and peak pressures. The data the iCare HOME2 generates help us monitor how patients respond to therapy, including postoperatively. This information supports why some patients experience disease progression while their IOP (based on in-office measurements) appears to be controlled.
Patients Who Benefit
It would be ideal to have an IOP profile of every glaucoma patient, but that’s not practical or reasonable these days. Instead, we focus on creating profiles of specific patients, particularly those who have pressure within normal range as measured in-office. We would expect most of these patients to be stable, yet they may not be. If a patient has some discernible glaucoma progression or other risk factors, we want to get a better idea of what their pressure is throughout the day.
When a patient comes in with a diagnosis of normal-tension glaucoma, we want to determine if it is truly that or if they are having IOP fluctuations that aren’t being captured in the office. To find out, we use the iCare HOME2 tonometer—and it’s impressive how often we learn that a patient with “normal” tension is actually experiencing a pressure spike early in the morning. These scenarios warrant a fresh look at the patient’s treatment plan.
Case 1: Treatment Based on iCare HOME2 Data Only
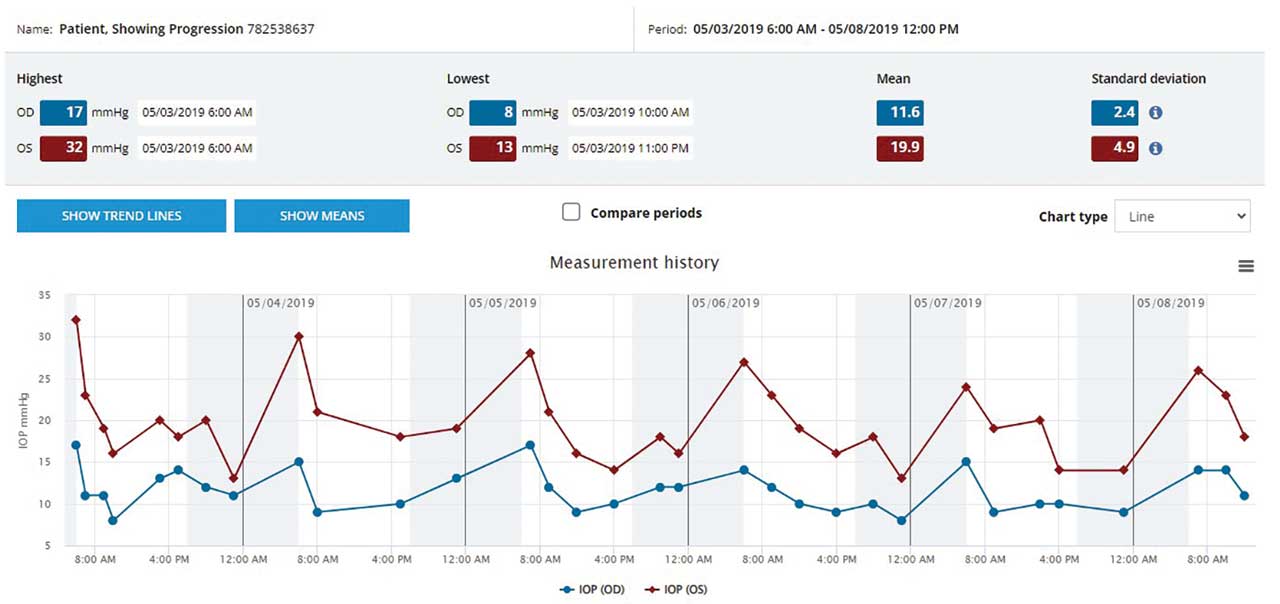
Our Approach to iCare HOME2 Monitoring
Goldmann applanation tonometry (GAT) is still the gold standard for IOP measurements. Studies have shown that measurements by iCare HOME, the predecessor of HOME2, are accurate and reliable and correlate well with GAT.3-5 What’s more, a recent study found that measurements using the HOME2 tonometer are interchangeable with those obtained with office based iCare tonometers.6
When we prescribe the iCare HOME2 tonometer to a specific patient, we do an assessment in the office to verify the correlation with GAT. Typically, the measurements are within one or two millimeters of mercury (mmHg), which is reasonable because we’re not looking at absolute numbers. We’re more interested in how the pressure readings are trending throughout the day. Knowing that the pressure rises in the morning or at different hours is more important than the absolute numbers.
Ideally, patients who use the iCare HOME2 measure their IOP five or six times a day over multiple days upon waking, throughout the day, at bedtime and even during the night. With these numerous data points to review, we can see diurnal IOP patterns and recognize day-to-day trends. We can look at the patient’s average IOP and any variations. If IOP increases at a certain time every day, we can be confident that we’re seeing a real pressure spike and not an artifact. Most importantly, we can look at peak pressure and what percentage of the time the pressure is above a certain target. This is valuable information that may influence our treatment plan going forward.
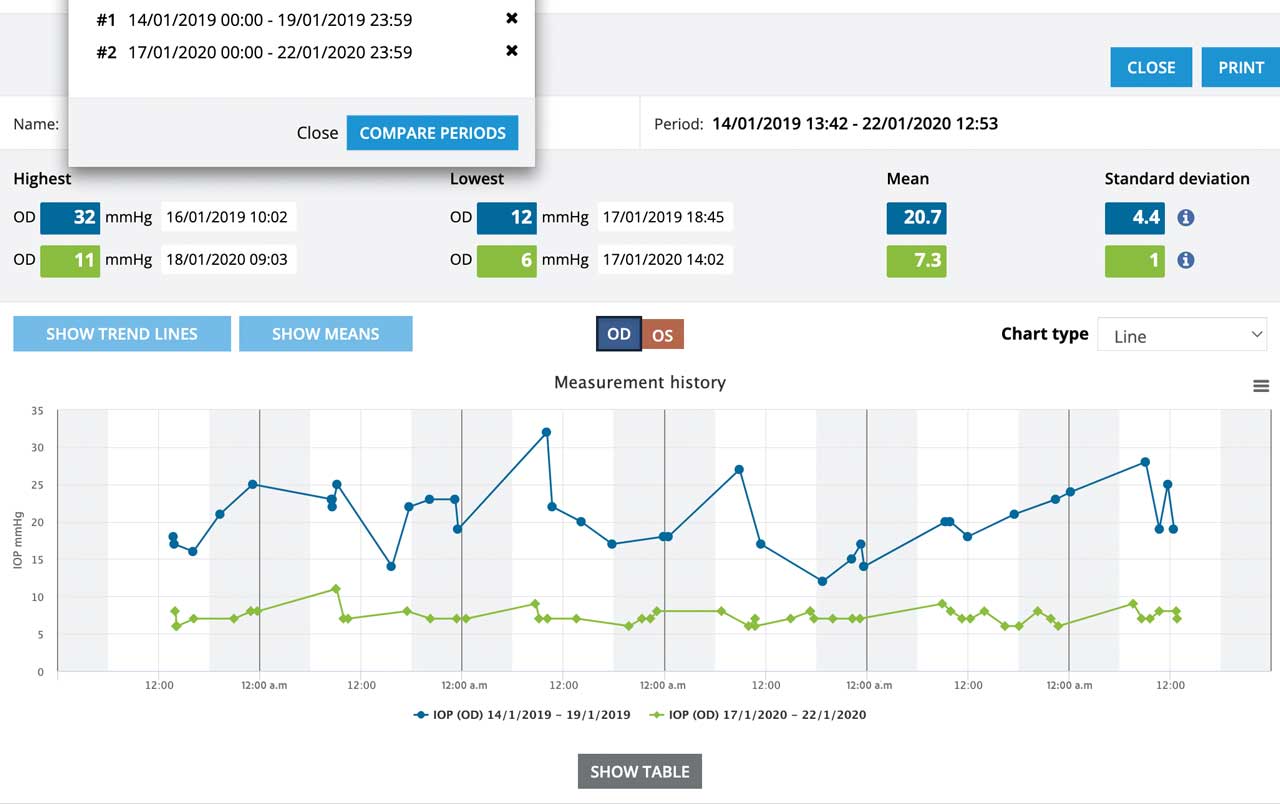
Case 2: iCare HOME2 Data Informs Therapy Decision to Prevent
Early Vision Loss in Young High-Risk Patient

Impact of Home Monitoring Data on Treatment
Data collected by the iCare HOME2 tonometer is an integral piece of a patient’s profile and can have a direct impact on the course of treatment. For example, take a patient who has normal-tension glaucoma but who is found to have a higher IOP reading at home than in the office. We would need to treat this patient to blunt those pressure elevations and then repeat the iCare HOME2 measurements to confirm that the treatment is effective. Absent the data from the HOME2, however, we would be trying to drive the patient’s pressure down to a very low number based on the in-office measurements.
Also consider patients whose disease is progressing despite normal pressures, forcing us to decide whether to perform a trabeculectomy or to use a less aggressive treatment, such as microinvasive bleb surgery or even a MIGS procedure. If the iCare HOME2 tonometer readings confirm the pressures are normal but the disease is progressing, we’ll know that trabeculectomy is necessary, despite its significant risks.
Conversely, we want to avoid high-risk procedures for patients whose pressures are within normal limits in the office but are spiking into the 20s at home; a less invasive therapy such as selective laser trabeculoplasty (SLT) will better control their pressure. Even though their pressures may change by only one or two millimeters of mercury, their peak pressures often drop by a larger amount, and that can make a difference for those patients.
These are just a few examples of how data from the iCare HOME2 tonometer help guide us in terms of diagnosis as well as selection of successful therapy.
Case 3: iCare HOME2 Shows Low IOP and Fluctuation Post-Trabeculectomy
Steps to Ensure Patient Acceptance
For the most part, glaucoma patients are in tune with their intraocular pressure. They understand that it’s important and that it can fluctuate, similar to those with high blood pressure who understand the importance of home monitoring or to diabetic people who wear glucose monitors. In each of these situations, monitoring is key to finding the right therapy to reduce the risk of disease progression.
The iCare HOME2 tonometer has an improved user interface, but there is a learning curve, so it’s important for patients to undergo training. Our technicians assist with this training, which takes about 20 minutes. We give patients specific instructions as to when they should take measurements (before and after instilling their drops, for example). We also provide literature that explains the measurement procedure, and iCare has produced an instructive video that shows, step-by-step, exactly how to use the HOME2 tonometer.
While some patients may opt to purchase this device, most patients in our practice rent an iCare HOME2 tonometer, usually for a week at a time. Patients typically return the device in good condition. They’re quite interested in our interpretation of their results and motivated to comply with their therapy.
Answer to an Unmet Need
As glaucoma specialists, we still do not have a solid grasp on which patients to treat more aggressively and which to observe. We don’t always understand what their target pressures need to be. There’s a lack of data, particularly when it comes to IOP.
The good news is that when patients measure their pressure at home throughout the day and night with the iCare HOME2, they capture crucial additional data: the timing, amount, and degree of pressure fluctuations, as well as peak IOP—all of which inform our approach to managing their disease.
Moving more toward 24-hour IOP monitoring will hopefully provide us with a better understanding of our patient’s IOP and disease progression. It can help us to determine target IOPs and to select the ideal therapy. The future of IOP assessment is beyond
single in-office measurements.
REFERENCES
1. Jonas JB, Budde W, Stroux A, Oberacher-Velten IM, Jünemann A. Single intraocular pressure measurements and diurnal intraocular pressure profiles. Am J Ophthalmol. 2005;139(6):1136-1137.
2. Asranwe S, Zeimer R, Wilensky J, Gieser D, Vitale S, Lindenmuth K. Large diurnal fluctuations in intraocular pressure are an independent risk factor in patients with glaucoma. J Glaucoma. 2000;9(2):134-142.
3. Termühlen J, Mihailovic N, Alnawaiseh M, Dietlein TS, Rosentreter A. Accuracy of Measurements With the iCare HOME Rebound Tonometer. J Glaucoma. 2016;25(6):533-538.
4. Cvenkel B, Velkovska MA, Jordanova VD. Self-measurement with iCare HOME tonometer, patients’ feasibility and acceptability. Eur J Ophthalmol. 2020;30(2):258-263.
5. McGlumphy EJ, Mihailovic A, Ramulu PY, Johnson TV. Home Self-tonometry Trials Compared with Clinic Tonometry in Patients with Glaucoma. Ophthalmol Glaucoma. 2021;4(6):569-580.
6. Realinwe T, Halenda K, Palko J, McMillan B, Balasubramanwe GK. Test-Retest Reliability of Intraocular Pressure Measurements with Office-Based versus Home-Based Rebound Tonometers. J Glaucoma. Published online May 27, 2024.
Iqbal Ike K. Ahmed, MD, is John R. and Hazel M. Robertson presidential endowed chair; professor of ophthalmology and visual sciences; and director of the Alan S. Crandall Center for Glaucoma Innovation, all within the John A. Moran Eye Center at the University of Utah, Salt Lake City. Dr. Ahmed also serves as the chief innovation officer and director of the glaucoma and advanced anterior segment surgery fellowship for the Prism Eye Institute in Ontario, Canada. He is a paid consultant for iCare and has received research funding from the company.
Anna Huixin Zhang, MD, is a research fellow and study lead coordinator with the glaucoma and advanced anterior segment surgery (GAASS) team at the Prism Eye Institute in Oakville, Ontario, Canada. She completed her medical training at Université Laval, Québec. Dr. Zhang has no conflicts of interest to disclose.
This content is sponsored by
![]()