






Modern cataract surgery increasingly aims to deliver precise refractive outcomes. Advances in optical biometry and intraocular lens (IOL) calculation formulas have significantly improved surgical planning and predictability. Despite these improvements, surgeons occasionally encounter a frustrating situation during preoperative evaluation: biometric measurements that simply do not agree.
Inconsistent measurements during cataract planning are often a signal that something within the ocular surface, cornea, or measurement process requires closer attention. In clinical practice, biometric variability is rarely random; more often, it reflects an underlying issue involving tear film instability, epithelial irregularities, subtle corneal pathology, or measurement conditions that deserve careful evaluation before proceeding with surgical planning.
As cataract surgery continues to evolve into refractive surgery, the tolerance for biometric error has become increasingly small. Even minor inaccuracies in corneal measurements can lead to significant refractive dissatisfaction, particularly in patients receiving toric or premium intraocular lenses.
When keratometry readings vary between scans or biometric data appear inconsistent, selecting the appropriate intraocular lens becomes more challenging and the risk of postoperative refractive surprise increases. Identifying the underlying cause of variability is often far more valuable than simply averaging discordant measurements. Recognizing the common causes of inconsistent biometry enables surgeons to improve measurement reliability and achieve more predictable refractive outcomes.
Start With the Ocular Surface
One of the most frequent causes of inconsistent keratometry readings is tear-film instability. Dry eye disease and meibomian gland dysfunction are highly prevalent among patients presenting for cataract surgery, particularly in older populations. When the tear film becomes irregular, the anterior corneal surface loses its optical smoothness, resulting in fluctuating keratometry readings between scans.
Even small variations in corneal curvature can significantly influence intraocular lens calculations, particularly in patients considering toric or premium intraocular lenses. For this reason, evaluation of the ocular surface should be one of the first steps taken whenever biometric measurements appear inconsistent.
Optimizing the Ocular Surface Before Repeating Measurements
When tear film instability is suspected, ocular surface optimization should be performed before repeating biometric measurements. Management may include:
-
Preservative-free artificial tears
-
Warm compresses and lid hygiene for meibomian gland dysfunction
-
Topical anti-inflammatory therapy such as cyclosporine or lifitegrast when indicated
-
Punctal occlusion in selected cases of significant aqueous deficiency
Once the ocular surface stabilizes, keratometry and axial length measurements should be repeated. In many cases, simply postponing surgery for a few weeks to optimize the ocular surface can dramatically improve measurement reliability and ultimately enhance refractive outcomes.
Look for Subtle Corneal Irregularities
Corneal pathology represents another important cause of inconsistent biometric measurements. Conditions such as epithelial basement membrane dystrophy, mild corneal scarring, early keratoconus, or subtle epithelial irregularities can alter corneal curvature and produce variable keratometry readings. These abnormalities may not always be obvious on routine slit-lamp examination, but they frequently become evident on corneal topography or tomography.
Role of Corneal Epithelial Mapping
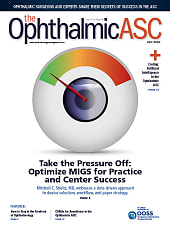
Advances in anterior segment optical coherence tomography (AS-OCT) now allow in vivo 3-dimensional mapping of the corneal epithelial layer, providing valuable insight into subtle corneal surface abnormalities (Figure 1).
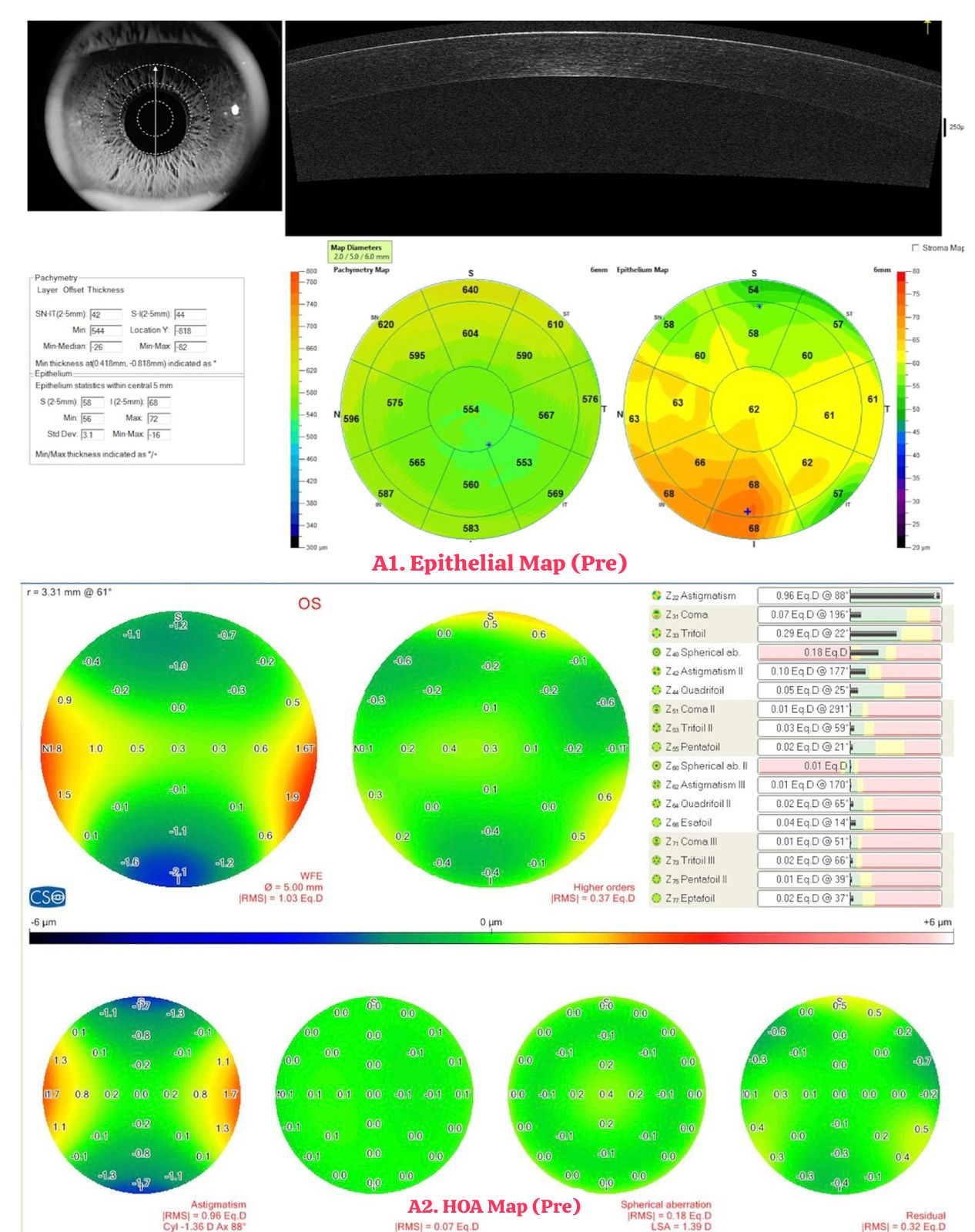
The corneal epithelium is a dynamic structure that continuously remodels in response to underlying stromal or surface irregularities. Variations in epithelial thickness can therefore mask or compensate for subtle corneal shape abnormalities that may not be detected by routine topography alone. For that reason, epithelial mapping has emerged as an important diagnostic tool in preoperative cataract evaluation, particularly in patients with unexplained variability in keratometry or inconsistent biometric readings. Figure 1a demonstrates an example of epithelial remodeling associated with ocular surface irregularity, while Figure 1b shows its improvement following ocular surface optimization.
Consider Measurement Conditions
Not all variability originates from ocular pathology. In some cases, measurement conditions themselves may contribute to inconsistent readings. Factors that may affect keratometry include poor fixation during scanning, blinking or tear film breakup during measurement, slight misalignment of the measurement axis, or an unstable tear film immediately before the scan. Ensuring proper patient positioning and allowing the patient to blink normally before each scan can help stabilize the tear film.
Consider Higher-Order Aberrations
In some patients, unexplained visual complaints or inconsistent visual quality may be related to higher-order aberrations rather than simple refractive error. Wavefront analysis and ray-tracing technologies can help differentiate whether optical aberrations originate from the cornea or the crystalline lens. Devices capable of separating corneal and internal aberrations allow surgeons to better understand the optical source of visual symptoms.
When Measurements Continue To Be Inconsistent
In some cases, biometric variability persists even after ocular surface optimization and careful measurement technique. Additional diagnostic tools can then be helpful.
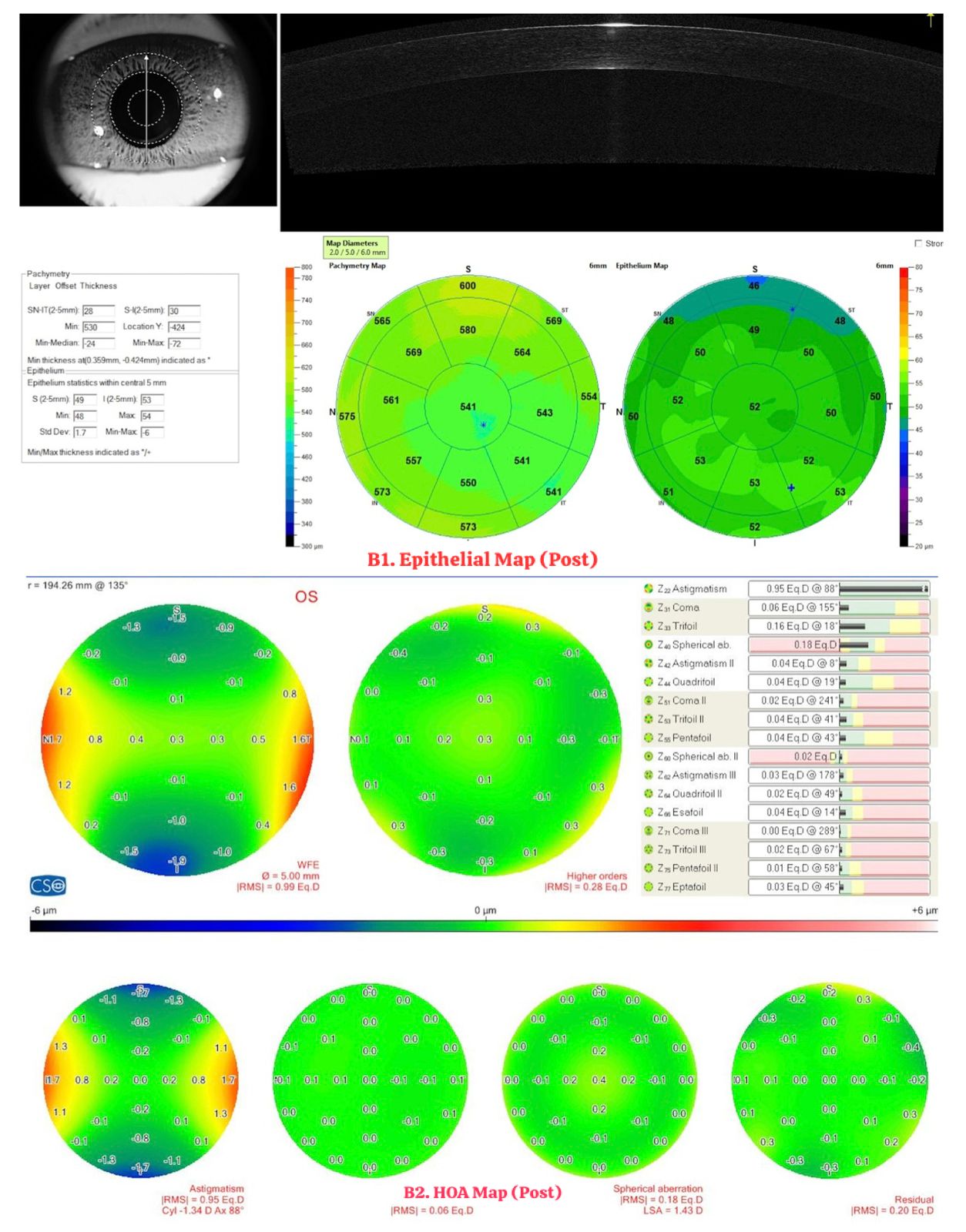
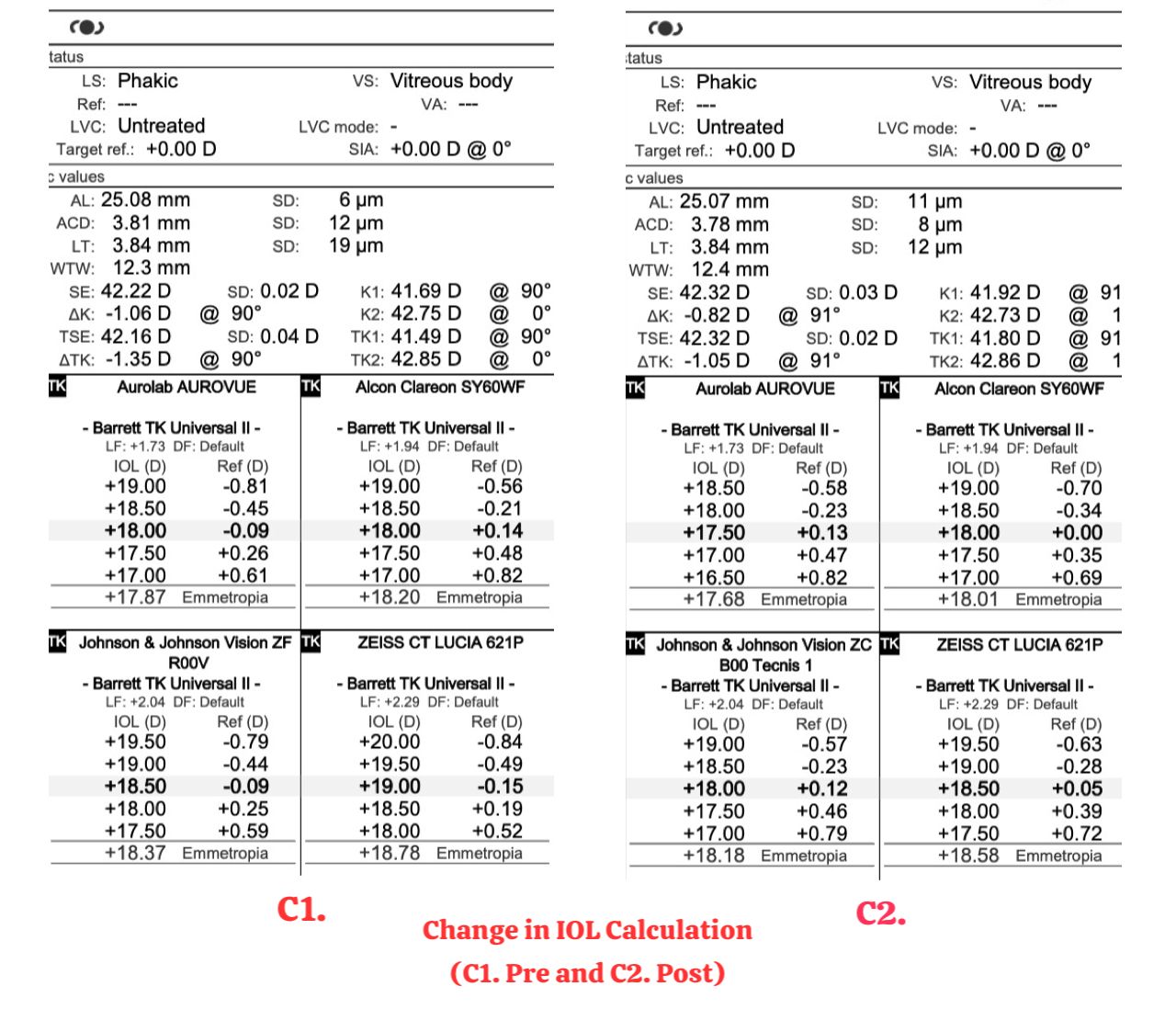
Corneal topography or tomography may reveal subtle irregular astigmatism or early ectatic disease that explains the variability. Comparing measurements from multiple biometric devices may also be useful. Stabilizing the ocular surface and improving measurement reliability may sometimes result in changes in calculated intraocular lens power (Figure 2).
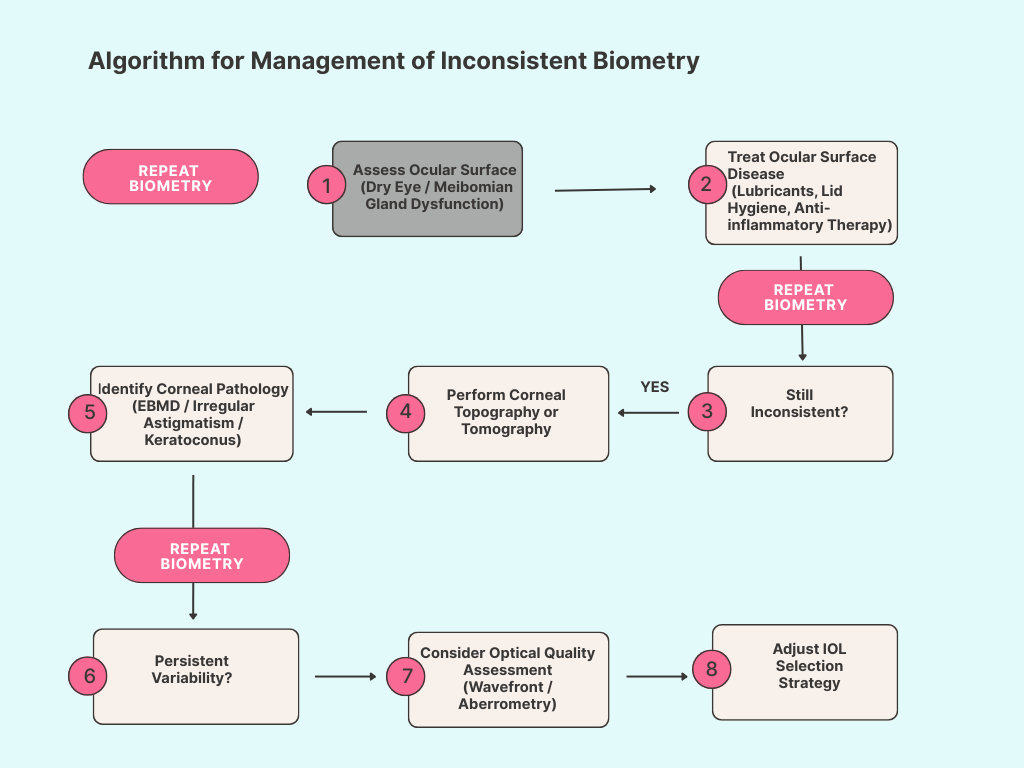
A Practical Workflow for Inconsistent Biometry
When biometric measurements do not agree, a systematic approach can help identify the underlying cause. The diagnostic workflow outlined in Figure 3 summarizes a practical approach to inconsistent cataract biometry.
Conclusion
Precise biometric measurements are fundamental to modern cataract surgery planning. When cataract biometry does not make sense, this variability often represents an important clinical clue rather than simply a technical problem.
By carefully evaluating the ocular surface, identifying subtle corneal irregularities, and optimizing measurement conditions, surgeons can significantly improve biometric accuracy and achieve more predictable refractive outcomes. Diagnostic tools such as epithelial mapping and wavefront analysis may further enhance our understanding of the optical system of the eye and guide more informed intraocular lens selection. When cataract biometry does not make sense, it is often worthwhile to pause, investigate the underlying cause, and repeat measurements rather than proceed with uncertain data.
Key Takeaways
Inconsistent biometric measurements are a common challenge in modern cataract surgery planning. A systematic evaluation of the ocular surface, corneal integrity, and optical quality can often reveal the underlying cause and help surgeons avoid postoperative refractive surprises.
-
Inconsistent keratometry readings are often the first clue to ocular surface disease.
-
Optimizing the tear film before repeating biometry can significantly improve measurement reliability.
-
Corneal topography or tomography should be considered when subtle corneal irregularities are suspected.
-
Corneal epithelial mapping can reveal surface irregularities that influence corneal refractive power.
-
Higher-order aberration analysis may help differentiate corneal from lenticular optical problems.
When measurements remain inconsistent, conservative intraocular lens selection may reduce the risk of refractive surprise.
